We demonstrate the safety and efficacy of a modified (scarless) orbital decompression technique to reduce eye prominence in thyroid and nonthyroid patients with shorter operative time and quicker recovery. Newer techniques and public demand have allowed such work to be done. Experience and expertise are critical in achieving safe results.
Key points
- •
Eye prominence (bulging eyes) can be a bothersome feature for some patients, both esthetically and functionally.
- •
Orbital decompression has long been used to reduce bulging eyes.
- •
Over decades, there have been several advances in orbital decompression technique with less and less invasive techniques designed.
- •
A modified (scarless) orbital decompression can reduce bulging eyes in esthetic (and nonesthetic) patients with quicker recovery.
- •
Experience and expertise are critical to achieve safe and effective results for orbital decompression surgery.
Esthetic orbital decompression
There are many people who are bothered by the appearance/prominence of their eyes and desire esthetic improvement; they complain, “my eyes don’t fit my face.” Although thyroid eye disease is a common cause of acquired prominent eyes, there are many other causes such as high myopic globes, shallow orbits with congenital proptosis, and congenital hypoplasia of the maxilla/zygoma, among other causes [ , ].
In addition to esthetic issue of prominent eyes for the patient, the patient with a relatively prominent eye presents a challenge to the surgeon planning esthetic or reconstructive surgery of the periocular tissues. When the globe is prominent relative to the orbital bony support, the eyelids lose mechanical advantage, and there is a tendency toward scleral show, lagophthalmos, tear pump dysfunction with epiphora, and descent of the eyelid–cheek complex, especially if/when these patients undergo traditional blepharoplasty. These disproportionate soft tissue bony relationships produce similar problems whether the proptosis is related to Graves disease, other active orbital process, enlarged globes (high myopia, buphthalmos, and so forth), congenital shallow orbit with congenital proptosis, or congenital hypoplastic malar eminence with sclera show [ , ].
Eyelid camouflage procedures that address the soft tissues alone, such as lateral canthoplasty, lower eyelid retraction surgery, and orbital rim onlay implants, can be used to camouflage the globe prominence but they are prone to failure if the underlying globe–orbit dystopia is not addressed [ , ]. They are simply suboptimal compared to repositioning the globe appropriately within the orbital space. Osteotomy and bony advancement is a substantially invasive option with significant morbidity than could address the globe–orbit dystopia but is obviously not preferred. The gold standard for treating prominent eyes is orbital decompression surgery.
Orbital decompression has had a long historical association with Graves exophthalmos because it is used to recess the globe relative to its bony support. However, orbital decompression has been shown to be of functional and cosmetic benefit to relative proptosis of nonthyroid origin, such as congenital shallow orbits, enlarged globes (high myopia, buphthalmos, and so forth), and hypoplastic malar eminence with sclera show, by recessing the globe relative to its bony support [ , ]. Regardless of cause, (relative) proptosis can represent a disfiguring problem for the patient with potential functional sequel in the aging process, especially for those who elect to undergo cosmetic eyelid surgery in the future.
To the credit of orbital surgeons, orbital decompression surgery has advanced tremendously during several decades, and a number of philosophic and technical advances have coalesced to evolve the surgical management of prominent globes. That includes the indications for orbital decompression, the bony surfaces that are selected for removal, and the incisions that are used to gain access to the orbital cavity. Orbital decompression surgery has evolved from a very invasive transcranial approach (with high morbidity and complications) to transantral Ogura approach (with high incidence of hypoglobus and diplopia) to more advanced eyelid crease and transcaruncular approaches with less morbidity, less complications, and quicker healing [ ].
As detailed in our earlier publication [ ], orbital decompression helps patients with prominent eyes, whether due to thyroid eye disease or congenital shallow orbits or maxillary hypoplasia or other, because they are bothered both esthetically and functionally. Furthermore, patients desire less invasive procedures/techniques with quicker recovery. Herein, we describe the safety and efficacy of a modified (scarless) customized orbital decompression technique to reduce eye prominence.
Technique
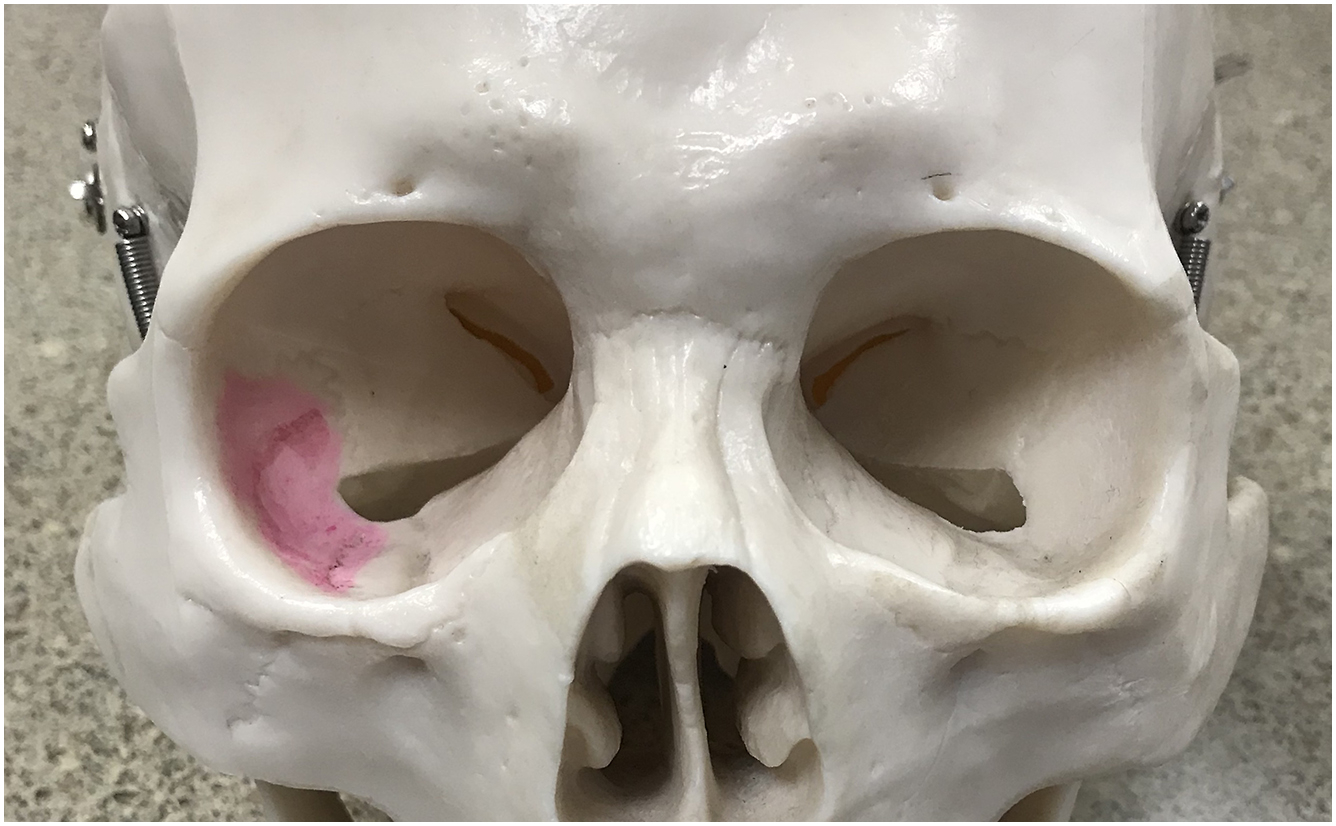
Preoperative CT scan was only used in suspicious cases. Orbital decompression is performed in graded customized fashion, based on the bony anatomy, amount of relative proptosis, the desired goal, and dynamic result of the surgery. Surgical technique for this modified (scarless) bony orbital decompression included lower eyelid transconjunctival approach to the inferolateral orbit area (mainly zygomatic bone), surrounding the inferior orbital fissure (inferior, lateral, and superior to) with/without fat removal. The conjunctiva is incised half way between inferior fornix border of the tarsus. The conjunctiva/retractors are then placed on upward stretch to protect the globe during the procedure. The periorbita is opened using steven scissors with spreading technique. Bone is removed at along the lateral orbital wall and lateral floor [ , ]. The fat is removed using blunt and sharp dissection with careful preservation of the muscles with enough fat covering them; see Figs. 1 and 2 and surgical [CR] . If additional orbital space is needed, medial orbital wall and posterior strut and medial intraconal fat is removed, in graded fashion, using a transcaruncular approach [ ]. Concurrent complimentary procedures (canthoplasty, infraorbital rim implants, and/or lower eyelid retraction surgery, periocular fat injection) are performed if deemed appropriate.