Craniosynostosis is a congenital condition characterized by the premature fusion of cranial sutures, disrupting normal skull and potentially brain growth. The current gold standard for nonsyndromic single-suture craniosynostosis is open cranial vault remodeling, which was pioneered by surgeons like Tessier and Whitaker in the 1970s. Recent advances have led to minimally invasive techniques, such as endoscopic-assisted strip craniectomy with helmeting, spring-assisted cranioplasty, and distraction osteogenesis. These methods aim to minimize surgical trauma, reduce blood loss, and shorten recovery times. This review assesses the evidence comparing open and minimally invasive surgeries for nonsyndromic single-suture craniosynostosis.
Key points
- •
Open surgical approaches to craniosynostosis are the historic gold standard, with reports of long-term shape and neurocognitive outcomes.
- •
Minimally invasive approaches to craniosynostosis reduce scar burden, reduce blood loss, and shorten recovery times.
- •
Long-term comparative studies on shape outcomes following open versus minimally invasive surgery are limited for nonsyndromic single-suture craniosynostosis.
- •
Long-term comparative studies on neurocognitive outcomes following open versus minimally invasive surgery are limited for nonsyndromic single-suture craniosynostosis.
- •
For rare conditions such as craniosynostosis, multicenter collaboration is necessary to find the best solutions for each diagnosis, phenotype, and patient.
Introduction
Craniosynostosis is a congenital anomaly characterized by the premature fusion of one or more cranial sutures, altering the natural growth pattern of the skull. , It can be broadly classified into syndromic and nonsyndromic types and occurs relatively frequently, affecting 1 in every 2000 to 2500 live births. , Craniosynostosis can be further categorized based on the involved cranial sutures: sagittal, metopic, coronal, or lambdoid, with a single suture or multiple sutures effected. Ultimately each diagnosis can cause a craniofacial deformity ( Table 1 ) with both a phenotype difference and a constrictive effect on brain growth, leading to possible developmental delay, increased intracranial pressure, or cognitive impairment.
| Deformity | Sagittal | Metopic | Unilateral Coronal | Unilateral Lambdoid |
|---|---|---|---|---|
| Predominant Skull Shape | Long and narrow skull, scaphocephaly, “boat shaped” | Trigonocephaly | Anterior plagiocephaly, forehead retrusion ipsilateral to fused suture | Posterior plagiocephaly, trapezium shape from vertex view |
| Anterior Cranium | Frontal bossing | Triangularly shaped forehead | Flattening ipsilaterally with contralateral frontal bossing, nasal root deviates ipsilaterally and nasal tip contralaterally | Contralateral frontal bossing |
| Orbital Deformity | — | Hypotelorism with retrusion of the lateral orbital wall | Harlequin deformity: ipsilateral orbit is narrow and tall, with superior displacement of ipsilateral lesser wing of sphenoid, ipsilateral raised eyebrow. Wide palpebral fissure | — |
| Middle Cranium | Reduced superior parietal width | Reduced bitemporal width | — | Ipsilateral mastoid bulge |
| Auricular Deformity | — | — | Ipsilateral ear displaced anterior and superior | Ipsilateral displaced posterior and inferior |
| Posterior Cranium | Occipital protuberance | Compensatory occipitoparietal widening | — | Parallelogram shape from posterior view, ridging on fused lambdoid suture |
Historic reports of craniosynostosis treatment centered on resecting the effected sutures, hoping this would permit normal brain growth. However, strip craniectomy alone often resulted in poor esthetic outcomes, failing to adequately address the cranial deformities associated with the condition. In the 1970s, the evolution of craniosynostosis treatment took a significant leap forward with the introduction of open cranial vault remodeling procedures. Pioneered by surgeons such as Tessier and Whitaker , these extensive operations demonstrated the safety and efficacy of reshaping the skull through direct manipulation of the cranial bones. Open cranial vault remodeling procedures became the standard of care, offering improved esthetic outcomes and the potential to prevent neurodevelopmental complications. However, these procedures were not without their drawbacks. They were typically lengthy operations associated with substantial blood loss, longer hospital stays, and high risk of complications.
In recent years, there has been a shift toward exploring and implementing more minimally invasive surgical techniques for the treatment of craniosynostosis. , Innovations such as endoscopic-assisted strip craniectomy combined with postoperative helmet therapy, , spring-assisted cranioplasty, , and distraction osteogenesis , have gained popularity due to their potential to reduce surgical trauma through smaller incisions, minimize blood loss, and shorten recovery times. These minimally invasive procedures offer a less invasive alternative to traditional open surgery, with the goal of achieving similar outcomes in terms of cranial shape and neurodevelopment ( Table 2 ).
Despite the growing interest in minimally invasive techniques, there remains a need for comprehensive evaluation of the comparative effectiveness of these approaches versus traditional open surgery. In this review, the authors analyze the current body of evidence comparing open and minimally invasive surgical options for nonsyndromic single-suture craniosynostosis by diagnosis, aiming to provide a balanced perspective on the advantages and disadvantages of each approach. Through this evaluation, they hope to highlight key considerations for surgical decision-making and identify areas where further research is needed.
Sagittal craniosynostosis
Sagittal craniosynostosis is the most common form of nonsyndromic craniosynostosis, representing 40% to 50% of these cases and occurring in approximately 1 in 5000 births. , It is characterized by the premature fusion of the sagittal suture, leading to the distinctive long and narrow skull shape, often associated with frontal bossing, occipital protuberance, and biparietal pinching, known as scaphocephaly.
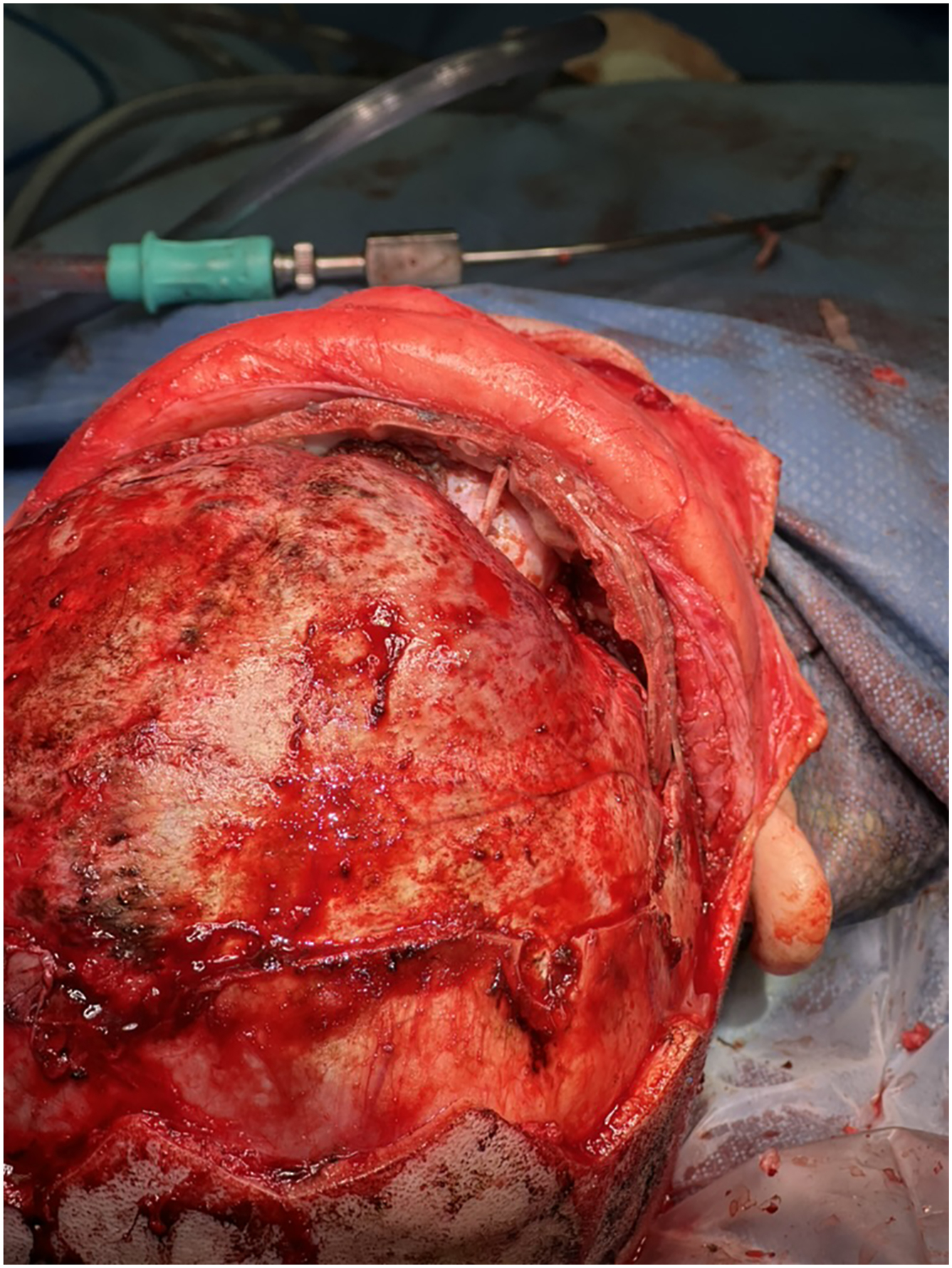
Open cranial vault remodeling is the conventional standard, well-established surgical technique for treating sagittal craniosynostosis. The procedure involves a large bicoronal scalp incision and extensive reshaping of the cranial bones. However, open cranial vault remodeling can differ significantly based upon the deformity and the surgeon or craniofacial center preferences. For instance, “total” cranial vault remodeling typically refers to reshaping the entire cranial vault, including the frontal, parietal, and occipital bones. However, this often requires the patient to be positioned in the sphinx position, which has been associated with increased venous air embolism risk, and involves longer duration. Middle and posterior vault remodeling addresses the deformities in the posterior two-thirds of the skull, anticipating compensatory improvement of the frontal bossing that typically occurs by the age of 2 years ( Fig. 1 ). Anterior vault remodeling via fronto-orbital advancement (FOA) focuses on the anterior half of the skull and the orbital bandeau and is typically used when the deformity is most concentrated in the frontal region or for correction of persistent frontal deformity at an older age.
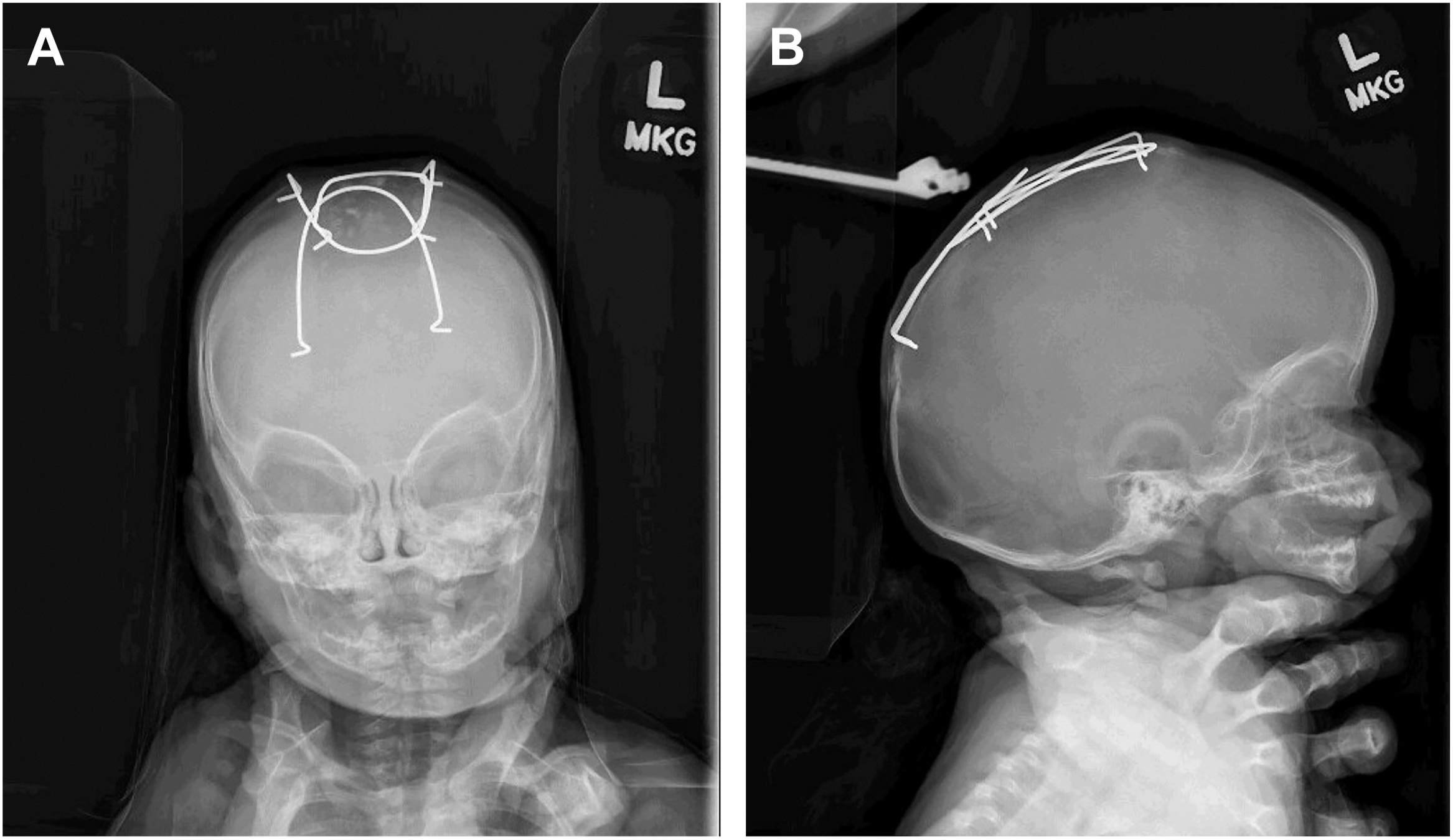
In contrast, suturectomy-based approaches involve smaller ostectomies performed at a younger age, typically through smaller incisions, and, at times, with the assistance of an endoscope. Brain growth alone is inadequate to correct cranial dysmorphology following suturectomy; a molding helmet, cranial spring, or cranial distractor is needed to facilitate reshaping. If molding orthosis is employed, the patient wears a custom-fitted helmet for 6 to 12 months to help mold the skull into a more natural shape. For spring-assisted surgery, a similar suturectomy is performed, and 2 to 3 springs are placed to gradually expand the cranial vault. These springs apply continuous outward pressure, allowing for controlled and progressive correction of the skull deformity ( Fig. 2 ). The springs are typically removed once sufficient reshaping has been achieved and the cranial defect is able to reossify after a few months.
Neurocognitive Comparisons by Technique
One of the critical considerations in choosing an intervention for any diagnosis is the potential impact on neurocognitive development. These outcomes are influenced by a multitude of factors, including genetics, phenotype severity, type of intervention, socioeconomic status, and family environment. As surgeons, we are constantly striving to perform the ideal intervention at the perfect age to maximize each patient’s outcome. Most teams will perform open surgeries aged around 9 months, while some prefer an older age at surgery seeking better shape outcomes, and others perform it younger seeking theoretically better neurocognitive outcomes. In an early foray into neurocognitive development in sagittal craniosynostosis, Speltz and colleagues found that there was no superiority of timing or type of procedure. However, intuitively age may play a role due to the evolving craniocerebral disproportion associated with diminished cranial growth, leading to the theory that earlier or more extensive procedures could result in superior neurocognitive outcomes. In a landmark study out of Yale University, Patel and colleagues found that those who undergo surgery at an age younger than 6 months have improved outcomes, leading the authors to favor early intervention. The same group followed up with a comparative study between 41 patients who underwent open cranial vault remodeling and 29 patients who underwent minimally invasive strip craniectomy and found superior neurocognitive outcomes following open surgery. However, they found no significant impact of age at time of surgery in this study. The Yale team has spearheaded a large volume of contemporary neurocognitive studies in patients with craniosynostosis, , although some methodologies employed and findings have been the subject of critical debate. For example, Derderian and colleagues noted that the average intelligence quotient (IQ) in the cohort treated with open surgery was 1.5 standard deviations above the national mean, suggesting that there may have been several neurocognitively bright outliers explaining the difference in the small sample size. They subsequently performed another comparative study between 36 patients who underwent open cranial vault remodeling and 39 patients who underwent spring-assisted cranioplasty and reported higher IQ and visuomotor integration scores following open surgery. However, Rogers and colleagues noted that the average IQ in the open surgery cohort was again 1.5 standard deviations above the national mean, higher than 83% percent of the population, calling the conclusions into question. A more recent multi-institutional, comparative study on 35 patients undergoing open repair, 46 patients undergoing minimally invasive repair, and 141 controls found no difference in cognitive outcomes by procedure.
Ultimately, disentangling the factors associated with neurocognitive development presents significant challenges, making it difficult to draw definitive conclusions about the superiority of any particular intervention. All methods for cranial vault expansion are reasonable options as long as they are performed in a timely manner.
Shape Outcomes
Cephalic index is the most commonly reported shape measure for sagittal craniosynostosis, as it simply computes the ratio between the cranial width and length. However, it is notably fraught with criticism, as it does not characterize many of the stigmatizing features of sagittal craniosynostosis. Several groups have described successful normalization of cephalic index following open and minimally invasive cranial vault expansion, , though there are only a few comparative studies. In 1991, Marsh and colleagues compared patients who underwent open surgery versus minimally invasive cranial vault expansion without helmeting and found better normalization in cephalic indices following open surgery. Thomas and colleagues also found improved cephalic indices following open surgery compared to strip craniectomy, though most patients in both groups normalized. Runyan and colleagues showed no difference in cephalic indices between open and spring-assisted cranioplasty. Lepard and colleagues found no difference in cephalic indices between open versus minimally invasive cranial vault expansion, though there was subjectively-rated esthetic benefits in the minimally invasive cohort. More recently, the group from Seattle Children’s Hospital compared patients who underwent minimally invasive cranial vault expansion with helmeting to age-matched and sex-matched patients who underwent open middle and posterior vault remodeling and found similar outcomes when looking at both cephalic index and more sophisticated 3 dimensional vector analyses. A systematic review and meta-analysis comparing open cranial vault remodeling, strip craniectomy, and spring-assisted cranioplasty found no difference in cephalic index between open surgery and springs, though there was a greater improvement in cephalic index with open surgery relative to strip craniectomy.
Thus, both open and minimally invasive approaches to cranial vault remodeling should produce acceptable esthetic outcomes if performed well, in a timely manner. However, as poorer preoperative severity predicts worse postoperative phenotypic severity, there may be suggestion that the most severe preoperative phenotypes would best benefit from open surgery.
Unicoronal Craniosynostosis
Coronal synostosis is the second most common form, accounting for 20% to 25% of nonsyndromic cases and occurring in roughly 1 in 10,000 births. , Patients with unilateral coronal craniosynostosis typically exhibit a characteristic flattening of the ipsilateral forehead with contralateral bossing, elevation of the ipsilateral orbital roof with a narrowing of the orbital width, and occasional nasal deviation (see Table 1 ). The head shape in vertex view is typically trapezoidal, due to ipsilateral posterior flattening and anterior positioning of the ear, compared to the classic parallelogram shape of positional plagiocephaly.
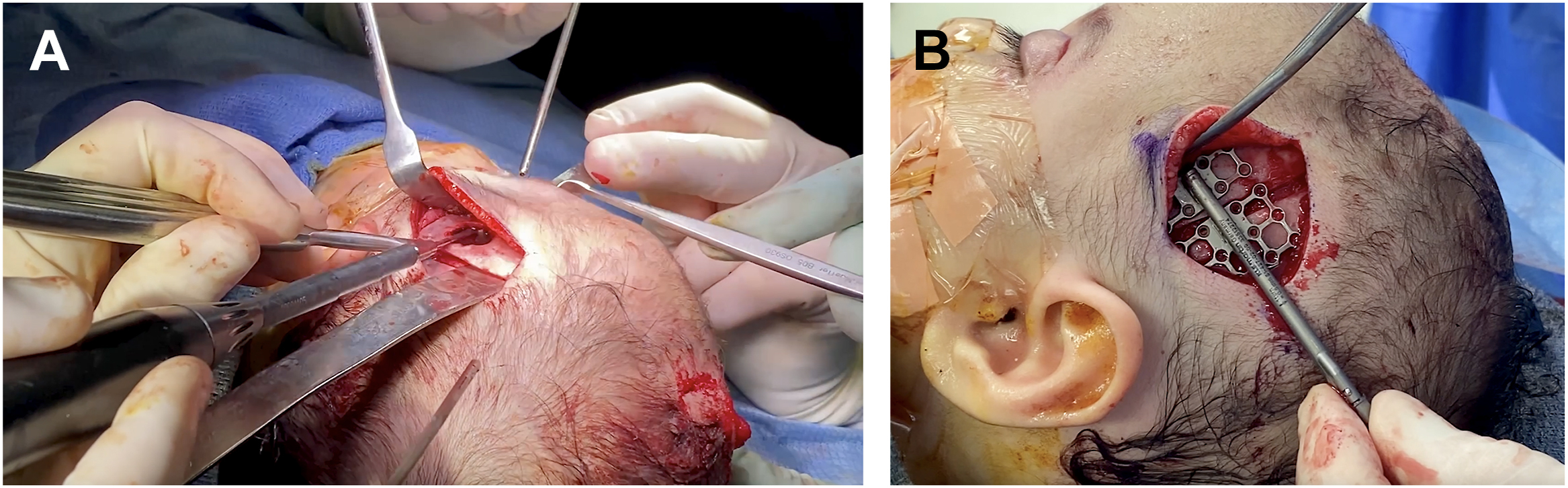
Open FOA has been the mainstay for cranial vault expansion and correcting the craniofacial deformities associated with coronal craniosynostosis. This technique involves a bicoronal incision with direct remodeling of the frontal bones and supraorbital bandeau such that the ipsilateral orbital rim is brought anterior and inferior to correct the Harlequin orbital deformity while the contralateral orbital rim is retruded. Depending on the phenotype and surgeon preference, surgery can also include ipsilateral superior orbital rim bone grafts to decrease the orbital height, contralateral interpositional orbital bone grafts to widen the contralateral orbit, and narrowing of the ipsilateral lateral orbital rim. Some surgeons perform bilateral bandeau advancement, whereas others advance primarily the affected side, hinging at the midline or at the contralateral orbit ( Fig. 3 ). This has also been performed using distraction osteogenesis following similar osteotomies on the ipsilateral fused suture, lateral calvarium, greater sphenoid wing, and orbital roof with a hinge osteotomy at the contralateral frontal bone. ,
Distraction osteogenesis has also been used in a minimally invasive approach, performing the same osteotomies and applying a cranial distraction device through 3 small incisions at the anterior fontanelle, ipsilateral pterion, and ipsilateral upper eyelid ( Fig. 4 ). Other minimally invasive approaches include endoscopic-assisted suturectomy followed by helmeting or spring-assisted surgery. One technical aspect of the procedure we believe critical particularly through minimal-incision approaches is adequate osteotomy and release of the advancing fronto-orbital complex from the sphenoid bone at the pterion; without release in this area, pterional retrusion persists postoperatively.
Neurocognitive Outcomes
There are no comparative studies focused on the neurocognitive outcomes between open FOA and minimally invasive surgeries. Some of the existing data on these outcomes suggest that there may be decreased mathematical and visual motor achievement associated with patients with unilateral coronal craniosynostosis, though these data are marred by the same limitations as described with sagittal craniosynostosis. A meta-analysis on 325 patients with unilateral coronal craniosynostosis suggested that these patients had below average neurodevelopmental scores, although scores generally remained within the normal range.
Shape Outcomes
At the advent of open craniofacial approaches to unilateral coronal craniosynostosis, there were centers which preferred a unilateral bandeau on the affected side versus a bilateral bandeau. Early studies suggested that for the majority of cases, either procedure would be appropriate, though in more severe cases with significant frontal bossing on the contralateral side, a bilateral bandeau would be preferable. However, as children with unilateral coronal craniosynostosis grew to skeletal maturity, surgeons, patients, and families noted a significant amount of forehead and supraorbital irregularity. Taylor and colleagues reviewed 238 patients with unilateral coronal craniosynostosis and found that only 10.2% had normal craniofacial esthetics at long-term follow-up. Most commonly, the abnormality was supraorbital retrusion followed by temporal hollowing, though only 22.7% of these patients underwent revisions that were either bone grafting to calvarial defects or only cranioplasty. They also found that overcorrection decreased the risk of temporal hollowing, leading some centers to “hypercorrect” in their surgical algorithm. A sophisticated 3 dimensional analysis out of Seattle Children’s Hospital found that an overcorrection of the bandeau resulted in 5 times the likelihood of having a symmetric result beyond 2 years postoperatively.
Thus, there is a fairly high degree of esthetic outcome variability following surgical intervention for unilateral coronal craniosynostosis. Endoscopic suturectomy with postoperative helmeting relies on early brain growth to push the skull into the correct position, while limiting the growth in other areas with the helmet. There are no comparative studies and there are minimal long-term data. Jimenez and Barrone showed excellent results, but this has not been reproducible in all centers. Dalle Ore and colleagues showed that 30% of their patients initially treated endoscopically later had to be converted to an open repair due to esthetic concerns. Domeshek and colleagues, Masserano and colleagues, and Teichgraeber and colleagues found no difference in the craniometric analyses between open FOA and endoscopic suturectomy with postoperative helmeting. Rather than relying on the brain to expand the calvarium, springs or distractor devices can also be used. One of the challenges with using springs in unicoronal cranial remodeling is limited control of the magnitude and vector of expansion. Distraction offers a controlled and more predictable way to correct the deformity but requires precise planning and execution to avoid malposition. , , , Additionally, maintaining dural and/or pericranial attachment to the frontal bone segment may reduce bone devascularization seen in other techniques, which may theoretically improve growth and decrease irregularities. Taylor and colleagues have reported endoscopic approaches to distraction osteogenesis, using pterional, anterior fontanelle, and upper blepharoplasty incisions.
While these techniques show promise and have theoretic advantages, shape comparisons between techniques are limited, and we do not have long enough follow-up on springs, distraction, or endoscopic strip craniectomy to provide consequential conclusions.
Metopic craniosynostosis
Metopic synostosis accounts for about 10% to 15% of nonsyndromic craniosynostosis cases and has an incidence rate of about 1 in 15,000 births. , Patients with metopic craniosynostosis typically exhibit a triangularly shaped forehead called “trigonocephaly,” a narrowed anterior cranial fossa, and often hypotelorism, or reduced distance between the eyes (see Table 1 ). The severity of the phenotypic expression can vary, though it is essential to distinguish between true metopic craniosynostosis and benign metopic ridging, as a closed metopic suture can be normal in infants. To aid clinical decision-making about severity and decision-making for operative treatment, machine-learning and artificial intelligence systems have been developed to calculate preoperative severity, such as CranioRate. , Some studies suggest that preoperative severity correlates inversely with postoperative appearance outcomes.
Open FOA is similarly the core procedure for cranial vault expansion and correction of the craniofacial deformities associated with metopic craniosynostosis. This technique involves a bicoronal incision with direct remodeling of the frontal bones and supraorbital bandeau, such that the interorbital distance is increased using a midline calvarial bone graft and the bandeau is reshaped so the lateral orbital walls form a more acute angle between the forehead and the temporal tenon ( Fig. 5 ). The goal is to primarily correct the forehead and orbital dysmorphology, while widening the anterior cranial fossa. Alternative FOA osteotomy patterns, such as the neo-frontobandeau procedure that transposes a parietal bone segment to create a single-segment fronto-orbital construct, are also used by our team in an effort to reduce some commonly seen late sequelae, such as frontal bony irregularity and retrusion.