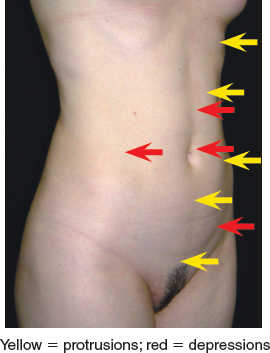
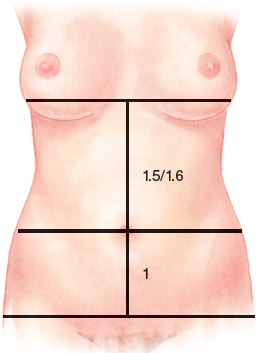
CHAPTER 8 Besides a thorough knowledge of classical anatomy and surgical techniques, plastic surgeons must understand the anatomy of corporeal beauty. Being able to recognize an aesthetically pleasing body contour allows one to diagnose a patient’s aesthetic pathology and to plan appropriate correction. Failure to perceive the nature of a patient’s less-than-ideal anatomy can lead to ineffective treatment; diagnostic errors are responsible for as many as one quarter of medical errors in plastic surgery. Fig. 8-1 Bozola and Psillakis stated in 1988 that a beautiful abdomen does not consist simply of a plane, but that it will have areas of relief. The reflection of light and shadow on the prominences and depressions of the abdomen creates a shape that resembles a lyre. The prominent areas are produced by the rectus muscles, iliac crests, pubis, hypogastrium, and inferior costal margins. The depressed areas are the supraumbilical median line, umbilicus, iliac fossa, and semilunar lines (the area from the oblique muscles to the rectus muscles). Fig. 8-3 Some parameters may guide plastic surgeons in the evaluation of the female abdomen. A vertical median line can be drawn from the pubis up to a horizontal line that intersects the submammary folds in the breast meridian. A normally positioned umbilicus divides the vertical line in a metric proportion of 1 on the inferior segment to 1.5 on the superior segment. Proportions of 1 to 1.4 or higher can be considered a high umbilicus. Presenting a short supraumbilical segment of skin, the proportions of 1 to 1.6 or less are considered a low umbilicus, presenting a long supraumbilical segment of skin. These factors are important in determining the skin resection necessary. The parameters of the waist and hips have a 1 to 1.5 proportion up to a 1 to 1.6 proportion. This had been long been considered the ideal form in historical literature, often called the golden section (Phi = 1 to 1.618). Phi and its role in harmonious proportions throughout the natural world have been studied and described for millennia by astrophysicists, botanists, architects, mathematicians, musicians, psychologists, physicians, dentists, and poets. We can find it in nature, and it was observed by Aristotle and Euclid in Greece in year 300 BC. In modern times British psychologist Chris McManus demonstrated its influence when observers of a collection of similar squares consistently chose figures that measured very close to the Phi proportion. Ricketts studied and applied Phi to the proportions of the human face. These authors claimed that when the Phi proportion exists within the segments of the face, the viewer’s limbic system is stimulated, and attraction occurs. A sense of beauty of the human form has been noted throughout time; it seems almost instinctual. Since 1982 I have been studying abdominoplasties. In 2010 I proposed the application of Phi proportion in relation to abdominal beauty, mainly in the position of the umbilicus. I contend that a low umbilicus, representing a value near Phi between the superior and inferior segments, makes for a more attractive abdomen. I have also applied the same theory to the breasts. In 1988 we proposed a new concept and classification for abdominoplasties, suggesting appropriate treatment for each deformity. Before this, all abdominoplasties were performed with resection of the infraumbilical segment of skin. With umbilical transposition, results were deemed poor because of excessive skin removal. The scars ultimately became large, high, or hypertrophic. They had an arc shape, with the concavity turned downward. Also, the lateral aspect of the scar crossed the inguinal fold toward the thighs, so the pubis became high, artificial, and separated from the abdominal anatomic unit, losing its sensuality and marring abdominal beauty. Postoperatively, these abdomens had an excessive stretch and always presented a high umbilicus and short supraumbilical segment of skin. Some authors proposed to perform the supraumbilical transverse incision first to detach the superior segment, stretching the abdominal flap toward the pubis and then marking the position of the transverse inferior incision. This was suggested to avoid the complications of excessively stretched skin, but the suprapubic transverse scar was usually very high in these cases. Sometimes a vertical scar was chosen (ending with a mini-inverted T scar), because some of the infraumbilical skin was kept within the flap to cover the abdomen. Was it was really necessary to keep that skin? Not in my view; what was required was a correct diagnosis of the patient’s deformity. There might be no skin excess, but the skin was removed. In such cases, a secondary surgery was necessary to lower the horizontal scar, but the vertical scar did not disappear. Consider the images of the patient above. The umbilicus was corrected through a reduction of its diameter. Part of the skin around the umbilicus was removed in a circumference shape, and the abdominal flap was stretched in its own direction. The resulting scar is little and vertical with a V-Y shape in its lower pole. The abdominal fat was not adequately corrected. Usually the adipose tissue under the fascia superficialis (lamellar layer) is removed from the infraumbilical area in a cone-shaped fashion in the region where the umbilicus is transposed. A thin narrow layer of adipose tissue in the supraumbilical midline is also removed. The anterior rectus sheath plication is always performed in the same way, regardless of the treatment of the adipose tissue. In our first study, as well as in follow-up reports, we proposed to classify patients in groups based on (1) skin excess, (2) subcutaneous tissue excess, (3) the degree of laxity of the myoaponeurotic layer, and (4) the position of the umbilicus on the abdomen, by dividing the abdomen in two segments, inferior and superior. By using this classification to guide our surgeries, the extent of skin removal was reduced, the scars became smaller and were placed lower, and it was possible to preserve the inferior shape of a lyre by stretching the skin with adequate tension. We were also able to avoid the separation of the abdominal anatomic unit from the pubic area. Today it is possible to remove enough skin to maintain the abdomen slightly stretched, the area of liposuction is ampler than before, and the muscular plication is performed using selective tunnels where the perforator vessels of the muscle are not located, or where they are not required to maintain good vascularization of the abdominal flap. Previously, the abdominal sensitivity was damaged as a result of significant undermining; now it is partially preserved. Mini-abdominoplasty is a world-renowned concept, but I think this term is not appropriate. Although in some patients with an abdomen that has a small amount of excess skin, it is possible to obtain a slightly smaller suprapubic scar; thus calling it a mini-abdominoplasty does not mean that it is a smaller surgery. With the evolution of liposuction, the treatment of the abdomen has changed and has become more comprehensive. Now abdominoplasties have been modified by a significant reduction of flap undermining with increased use of liposuction, associated with tunneling in areas without important perforator vessels so that the myoaponeurotic layer can be accessed to perform the aponeurotic plication. There has also been a reduction of the extent of skin removal and traction. The attachment of the flap to the aponeurosis is another improvement that has lowered the incidence of seromas. Clearly, there is nothing “mini” about this technique. The Bozola and Psillakis classification (1988) contributed to surgeons’ understanding that different diagnoses in the same body area can demand different treatments. Ultimately, we proposed five different groups, as listed in the table, with their respective treatments for aesthetic deformities of the abdomen. ■ During vibroliposuction, the main risk is perforation of the abdominal cavity, so the surgeon must exercise caution when performing this procedure. ■ The vibrolipoaspiration of the superior abdomen has to be performed in the craniocaudal direction using the cannula opening over the xiphoid process. Therefore it is possible to avoid transfixion to the wall under the ribs. ■ The patient cannot stay in the ventral decubitus for long, because a perforation of the renal area and vascular alterations could occur when the patient returns to the dorsal decubitus position again. ■ The plications/plicatures of the aponeurosis are performed through small underminings that preserve the maximum axial circulation of the skin and the subcutaneous region that are originated from muscle perforator vessels to avoid necrosis. At present I have operated on and followed more than 500 abdominoplasty patients, and the tactics, techniques, and statistics that I describe in this chapter are the result of this experience. I continue to employ the principles of this classification system, but I have adopted new techniques such as vibroliposuction equipment (power-assisted liposuction [PAL]). Vibroliposuction is a kind of liposuction that the cannula of the equipment moves by compressed air, and the surgeon can handle it gently, so it increases the productivity of the surgery. I have implemented some changes in my procedure, such as performing a more extensive liposuction; the undermining is now performed in tunnels. My approach now encompasses a more inclusive area of treatment during abdominoplasty, correcting more than just the anterolateral aspect of the abdomen. I strive to treat the entire trunk circumference, from the inframammary fold to the inguinal crease, including the lower flank, the superior part of the buttock, the lumbar area, and the inferior portion of the thorax (hypochondrium). By using these principles, I am able to achieve a more natural shape of the abdomen and trunk. Next I will address specific considerations for the five groups of the classification. Liposuction of the abdomen is performed with the patient in the Trendelenburg position. It is not necessary to change to the decubitus position to access the flanks and lumbar region, because this may result in complications from hemodynamic changes. So that the flanks and lumbar region can be treated on the right side, the right leg should be crossed over the left leg, thus forcing the trunk laterally. Then the patient’s legs are crossed the opposite way for access to the left side. The operating room must have a temperature above 20° C (68° F), because body temperature decreases during surgery, which may cause a reduction in blood flow to the lower limbs, thus increasing the risk of thrombosis. The surgical site is infiltrated with 2 L of a hyposmolar solution, which is composed of 1000 ml of saline solution, 1000 ml of distilled water, 10 mg of dexamethasone, and 2 ml of epinephrine in a concentration of 1:1000, and 5000 IU of hyaluronidase. The patient remains under general anesthesia, with the blood pressure kept 20% lower than the baseline preoperative value. Liposuction is performed using a PAL device, with 3 or 4 mm cannulas. A 0.5 cm incision is made at the xiphoid process, the iliac fossa, on the flanks, and, when necessary, in the hypochondrium. At the beginning of the surgery, 1 g of intravenous hydrocortisone is given; at the end of the surgery, 10 mg of dexamethasone is also infused. In cases of large areas liposuctioned, an extra dose of 4 mg dexamethasone may be used 12 and 24 hours after the operation. In plastic surgery, the corticosteroid is used to reduce edema and inflammation, which could decrease the quality of the final result. With extensive inflammation of the vascular endothelium, antithrombin and reactive C protein are produced, resulting in a hypercoagulable state. More extensive and longer procedures increase the stress generated by surgery. In such cases a more intense inflammatory reaction is generated, with consequent activation of the blood coagulation system, without the natural inhibitory action of the endothelium. Any kind of tissue trauma that affects 20% of the body area (as in burned or injured patients or those undergoing liposuction or extensive surgery) can be considered severe and causes a systemic inflammatory response syndrome (SIRS), resulting in changes in the equilibrium of blood hemostasis. This results in an increased risk of thrombosis. PAL is performed in all layers of the adipose tissue, preserving 0.5 to 1.0 cm of the most superficial layer. The regions treated are those that will be enhanced by more depression, creating areas of light and shadow while respecting the lyre shape described previously. Compressive garments are placed on the patient while she is still under general anesthetic, with blood pressure 20% lower than baseline. This patient is instructed that the garment can be removed every day for showering. The garment must be worn for 2 months. Patients are kept with their bodies in the Trendelenburg position in the intraoperative and postoperative periods. Also, the patients have to keep their legs elevated until they are able to resume their routine activities. Placing a suction drain is not necessary in group II patients. For other groups a suction drain may be necessary, but attaching the flap on the aponeurosis can help to avoid or reduce the length of time a drain is required. Local and/or systemic complications can occur in abdominoplasties. Local complications are related to skin, subcutaneous fat, muscle aponeurosis, and umbilicus. Large underminings of the abdominal flap and excessive stretch of the skin can lead to necrosis, because it will not remain skin to realize future corrections. Wide and/or hypertrophic scars, keloids, hyperchromia, hypochromasia, stenosis of the umbilicus, and a wrong position of the scars can damage the final result, presenting an inappropriate anatomy. Infections lead to flap necrosis and postoperative surgical suture dehiscense. A disseminated infection in the undermined areas in the tunnels of the vibrolipoaspiration causes toxemia and toxemic shock. Hematomas and seromas can come from the undermined abdominal flap. They produce excessive fibrosis that contracts and leads to skin archings. The more common systemic complication is deep venous thrombosis and its consequences. The surgeon should not return to the same region twice to perform liposuction, because clots may be suctioned, causing the area to bleed again. This procedure is performed only in restricted cases when few regularizations of subcutaneous surfaces are needed. A common complication in patients of groups II and III is that a transverse fold outlining the umbilicus is formed, creating a so-called sad-face scar. There are three alternatives to deal with this complication: 1. A half-moon shaped section of skin approximately 2 cm wide is excised above the umbilicus, elevating its superior half and creating a half-moon scar. 2. The infraumbilical flap is undermined up to the umbilicus pedicle; this pedicle is cut and reimplanted right below its original position with a bolster stitch point (as in group IV patients). 3. The umbilicus is released from the flap, leaving it attached to the aponeurosis, and after flap traction and resection, an omphaloplasty is performed in the same way as in group V patients, and the wound is closed by layers, leaving an infraumbilical vertical scar almost always starting from the umbilicus.
Mini-Abdominoplasty: Classification and Treatment
Surgical Anatomy

THE PHI PROPORTION: THE GOLDEN RATIO
A New Classification for Abdominoplasties
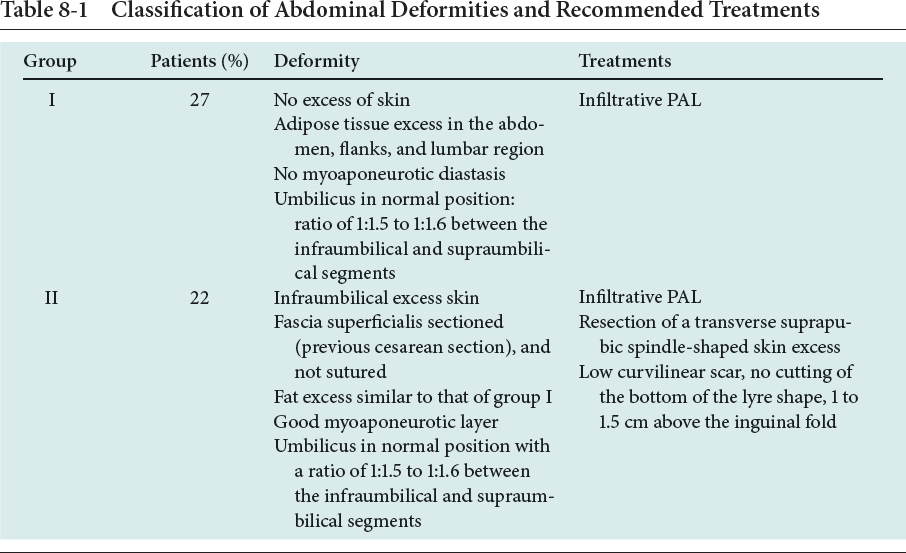
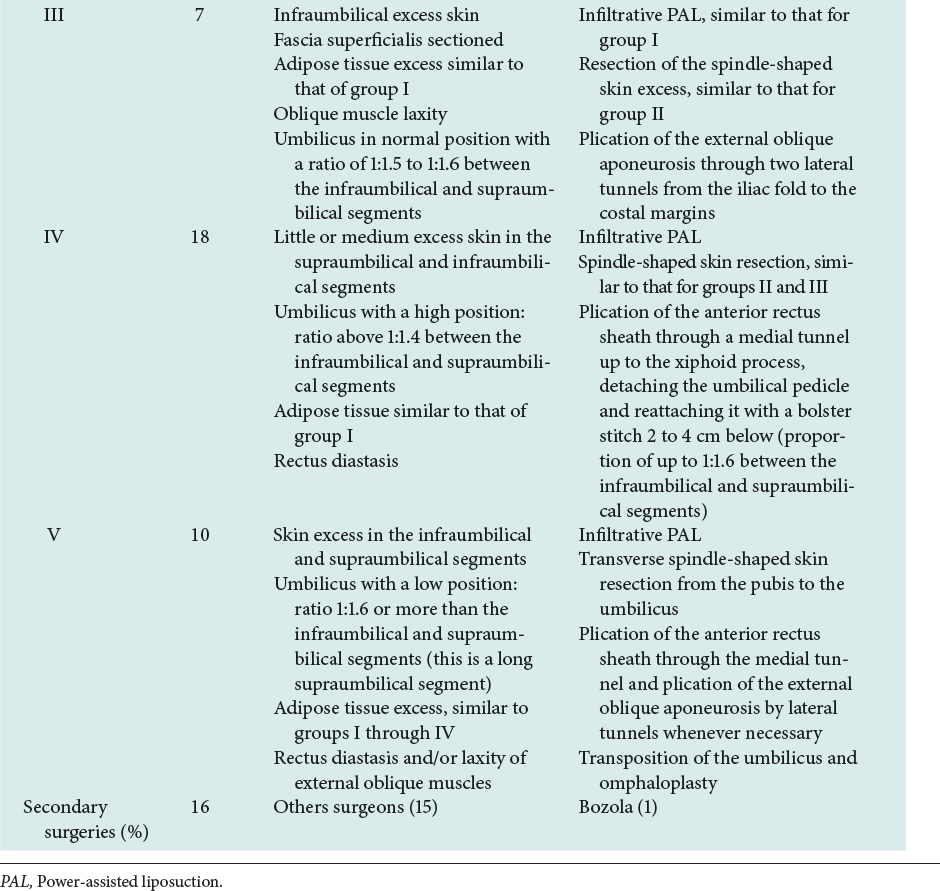
Abdominal Classification of Aesthetic Pathologies and Their Respective Treatments
PATIENT POSITIONING
ANESTHESIA
TECHNIQUE
POSTOPERATIVE CARE
PROBLEMS AND COMPLICATIONS
GROUP I
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine