Alloplastic malar augmentation offers a reliable means of achieving a permanent, yet reversible, form of midfacial volume enhancement that serves to correct the changes associated with facial aging, hypoplasia, and congenital malar asymmetry. The degree of augmentation depends on the severity of existing malar bony hypoplasia, soft tissue volume loss/ptosis, or both. Facial aesthetic surgeons have a multitude of implant designs and shapes and implant materials available. The transoral surgical approach with transcutaneous implant suture stabilization is the most commonly used surgical protocol in alloplastic midface augmentation and is, therefore, the technique specifically chosen for review in this article.
Key points
- •
Alloplastic malar augmentation provides a permanent yet reversible form of midfacial rejuvenation that can be tailored to patients’ anatomy.
- •
Malar deformities can be categorized into types I, II, and III, depending on the presence of bony malar hypoplasia, submalar soft tissue volume loss/ptosis, or both, respectively.
- •
Choosing the correct implant design is essential in achieving ideal malar augmentation. A combination of malar, submalar, and malar-submalar implant shapes are available.
- •
The surgeon should thoroughly inspect the face for the presence of any significant preexisting facial asymmetries before determining the type and size of implant to be used.
- •
The transoral surgical approach allows for rapid and precise placement of malar implants. Implant stabilization in the immediate postoperative period is necessary to minimize the possibility of implant displacement.
Introduction
The malar region may be considered the most important facial region imparting a youthful countenance to the human visage. The combination of the underlying bony support, adipose tissue, and mimetic musculature generates a dynamic dimension to the face that is essential for the beauty of human expression and facial balance. Such a delicate arrangement is prone to deformation because of the ever-present forces of aging, gravity, solar radiation, and bodyweight fluctuations. Over time, even a full malar pad becomes ptotic and atrophic, leading to the withered appearance characteristic of senescence. The presence of additional congenital malar bony deficiency accentuates such aging changes and may even act to accelerate them.
Presently, the modern facial aesthetic surgeon has an available surgical and nonsurgical arsenal that is unmatched compared with any other period in the history of our field. According to the American Society of Plastic Surgeons, as of 2013, hyaluronic acid augmentation of the face has risen to become the second most commonly performed nonsurgical procedure in the United States, behind only botulinum toxin, with nearly 2 million procedures performed yearly. Such rapid growth and widespread use have been fueled by a need to create a more balanced, fuller, and, therefore, youthful facial harmony via augmentation of the cheeks. Despite this, injectable midface augmentation has shown limitations with durability, permissibility of large-volume augmentation, and correction of bony malar deficiency without imparting an adynamic or bloated-face appearance. Alloplastic augmentation provides a durable yet reversible form of malar augmentation that lends itself well to a significant proportion of patients seeking midfacial volume enhancement. This article describes the intrinsic details inherent to alloplastic midfacial augmentation, with procedural details describing the most commonly used surgical technique in current use.
Introduction
The malar region may be considered the most important facial region imparting a youthful countenance to the human visage. The combination of the underlying bony support, adipose tissue, and mimetic musculature generates a dynamic dimension to the face that is essential for the beauty of human expression and facial balance. Such a delicate arrangement is prone to deformation because of the ever-present forces of aging, gravity, solar radiation, and bodyweight fluctuations. Over time, even a full malar pad becomes ptotic and atrophic, leading to the withered appearance characteristic of senescence. The presence of additional congenital malar bony deficiency accentuates such aging changes and may even act to accelerate them.
Presently, the modern facial aesthetic surgeon has an available surgical and nonsurgical arsenal that is unmatched compared with any other period in the history of our field. According to the American Society of Plastic Surgeons, as of 2013, hyaluronic acid augmentation of the face has risen to become the second most commonly performed nonsurgical procedure in the United States, behind only botulinum toxin, with nearly 2 million procedures performed yearly. Such rapid growth and widespread use have been fueled by a need to create a more balanced, fuller, and, therefore, youthful facial harmony via augmentation of the cheeks. Despite this, injectable midface augmentation has shown limitations with durability, permissibility of large-volume augmentation, and correction of bony malar deficiency without imparting an adynamic or bloated-face appearance. Alloplastic augmentation provides a durable yet reversible form of malar augmentation that lends itself well to a significant proportion of patients seeking midfacial volume enhancement. This article describes the intrinsic details inherent to alloplastic midfacial augmentation, with procedural details describing the most commonly used surgical technique in current use.
Treatment goals and planned outcomes
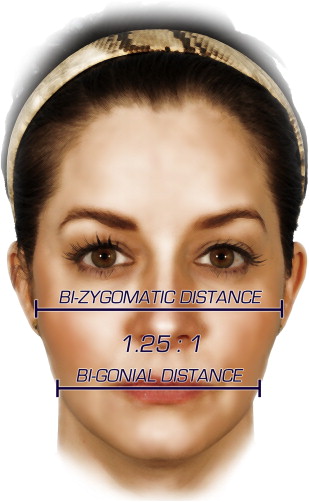
The primary goal of alloplastic midface augmentation is to attain a permanent volumetric enhancement of one or more components of the malar region, with a secondary endeavor to achieve an improved degree of facial symmetry. Anatomically, the malar eminence is the most protuberant bony prominence of the midface and represents the body of the zygomatic bone, which can be easily palpated on physical examination. The presence of bony hypoplasia imparts a certain degree of flatness to the human face that can be easily identified and should be carefully noted preoperatively. Measuring the bizygomatic distance on a frontal view can aid in the identification of malar hypoplasia, as that value typically exceeds the bigonial distance by 25% to 30% in patients with aesthetically balanced faces ( Fig. 1 ).
A second distinct region of the midface, the submalar triangle , is defined as the region bordered superiorly by the malar eminence, medially by the nasofacial fold, and laterally by the masseter muscle. This region is essential to consider before cheek augmentation, as this region’s apparent fullness primarily depends on its soft tissue content, in particular the malar fat pad. During the process of natural aging or in those affected by lipodystrophy of the midface, the submalar triangle undergoes significant volume loss secondary to adipose tissue atrophy and/or midfacial soft tissue ptosis. The presence of significant submalar volume loss indicates the need for a cheek implant design that specifically augments this region.
Patients seeking malar augmentation have previously undergone multiple rounds of cheek volume enhancement via injection with one of the currently available temporary fillers. Often, these individuals prefer the convenience and cost-effectiveness of a one-time procedure for long-lasting augmentation. Surgically, the placement of a solid implant directly on a hypoplastic bony malar region also yields a more natural result that easily achieves a high degree of aesthetic enhancement. Despite these truths, the aesthetic facial surgeon should consider a multitude of patient and implant features before recommending this procedure to cosmetic patients.
Preoperative planning and preparation
Implant Design
The extent of the midfacial augmentation as it relates to implant shape and size largely depends on the physical examination findings and the apparent degree of bony and soft tissue deficiencies of the malar region. As originally described by Binder, 3 types of midface deformity can exist, which are classified into types I, II, and III ( Fig. 2 ). Individuals with a type I deformity display a certain degree of malar bony hypoplasia but otherwise have relatively normal midfacial soft tissue volumes. Type I patients benefit from the insertion of a malar- type implant ( Fig. 3 ). Patients with a type II deformity, the most commonly encountered form, have normally projecting malar bony eminences but demonstrate considerable midfacial soft tissue loss caused by fat atrophy and/or malar ptosis, often secondary to the aging process. These patients require the insertion of a submalar -type implant, which specifically augments the submalar triangle (see Fig. 3 ). Finally, those with a type III midface deformity have a combination of both malar bony hypoplasia and soft tissue loss or ptosis. Type III individuals benefit most from a combined malar-submalar –type implant (see Fig. 3 ). Once the ideal implant design is chosen, the surgeon should next determine which implant material to use.

Related posts:
 Midface and Periocular Rejuvenation
Brow/Upper Lid Anatomy, Aging and Aesthetic Analysis
Endoscopic Midfacial Rejuvenation
Midface and Periocular Rejuvenation
Brow/Upper Lid Anatomy, Aging and Aesthetic Analysis
Endoscopic Midfacial Rejuvenation
 Avoiding and Managing Complications in the Periorbital Area and Midface
Endoscopic Midfacial Rejuvenation
Avoiding and Managing Complications in the Periorbital Area and Midface
Avoiding and Managing Complications in the Periorbital Area and Midface
Endoscopic Midfacial Rejuvenation
Avoiding and Managing Complications in the Periorbital Area and Midface
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


