The Clinical Problem ( Fig. 8.1 )
Rejuvenation of the midface was formerly limited to a lower lid blepharoplasty in conjunction with some form of a face lift. Neither adequately addresses the nasojugal groove (also referred to as the tear trough) or the nasolabial fold. Furthermore, a traditional lower lid blepharoplasty would frequently include resection of herniated lower lid fat, which in turn could produce a gaunt, deflated lower lid that does not appear youthful.

Recently, more attention has been given to restoring a youthful look to the midface by volumizing the face and avoiding resection of lower lid fat as we have recognized the loss of periorbital fat as part of the aging process.
The Aesthetic Problem
Our patients present complaining of “looking tired,” “bags under my eyes,” or “dark circles under my eyes.” What they are describing in popular terms are the classic aging changes that are manifest in the lower lids and middle third of the face. These include the following:
- ▪
Loss of skin laxity, leading to excess lower eyelid skin and fine wrinkles
- ▪
Midface descent and ptosis of the malar soft tissues
- ▪
The appearance of two aesthetic units—that is, the lower lid and cheek are demarcated by the tear trough, where there was only one in the person’s younger years
- ▪
Increase in the vertical dimension of the lower lid—lid margin to tear trough distance
- ▪
Fat herniation
- ▪
In its most severe form:
- •
Lateral canthal dystopia
- •
Scleral show
- •
Poor lower lid tone, ectropion
- •
Management and Treatment Options
Our goal is to restore the youthful appearance to the midface and should therefore ideally correct or at least improve the problems noted above:
- ▪
Resect redundant lower eyelid skin.
- ▪
Resuspend the malar soft tissues.
- ▪
Blunt or eliminate the tear trough, restoring a single aesthetic unit.
- ▪
Decrease the vertical dimension of the lower lid.
- ▪
Preserve volume.
- ▪
Correct canthal dystopia if present.
There are many options available to rejuvenate the midface. A comprehensive historical review nicely outlines the various techniques being used today.
The transblepharoplasty subperiosteal cheek lift is my preferred approach. Although it could be argued that it is technically more demanding than a traditional lower lid blepharoplasty, it successfully addresses the midface descent and aims to blunt the tear trough, neither of which is adequately corrected by a lower lid blepharoplasty alone.
Surgical Preparation and Technique
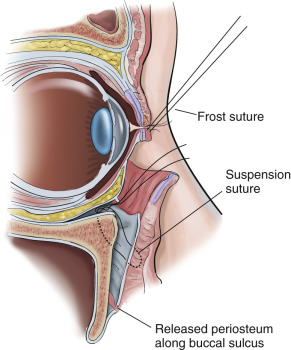
The procedure is performed under general anesthesia. A subciliary incision is marked with brilliant green and infiltrated with a solution of 1% xylocaine, with 1 : 100,000 epinephrine. The cheek is also infiltrated but is not tumesced. Corneal protectors are inserted with an ocular lubricant (e.g., Lacri-Lube) and/or tobramycin and dexamethasone ophthalmic ointment (e.g., Tobradex). A 4-0 silk Frost suture is used for countertraction. After allowing the vasoconstriction to take effect, the subciliary incision is made and a skin muscle flap is developed in the preseptal plane, all the way to the infraorbital rim. The arcus marginalis is incised and a subperiosteal dissection of the entire cheek is performed while protecting the infraorbital neurovascular bundle. Dissection proceeds in a subperiosteal plane over the nasomaxillary buttress, anterior maxillary wall, malar eminence, and lateral orbital rim to the anterior third of the zygomatic arch.
The periosteum is released inferiorly just above the buccal sulcus as well as over the masseteric fascia, thus allowing mobilization of the entire cheek in a superior temporal vector, more or less perpendicular to the nasolabial fold. This maneuver should produce a 5- to 8-mm (sometimes more) redundancy of periosteum above the lateral portion of the infraorbital rim.
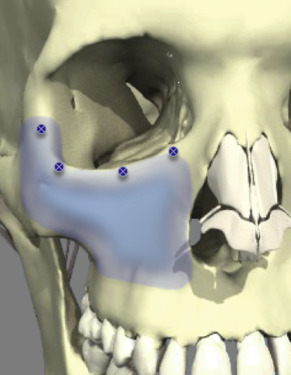
Four 1.1-mm drill holes are placed along the infraorbital rim, as shown in Fig. 8.2 . One drill hole is medial to the level of the infraorbital foramen, and the other three are at the midportion of the infraorbital rim, the lateral corner, and the lateral canthal level.
Then, 3-0 Ethibond sutures (Ethicon, Somerville, NJ) are used to suspend the periosteum along with the entire cheek soft tissue envelope in a superior-temporal vector ( Fig. 8.3 ). Care must be taken not to overdo this suspension because it can produce an unnatural appearance.
A lateral canthopexy is usually not performed unless the patient requests that her or his lateral canthi be raised, or there is significant lower lid ectropion and scleral show preoperatively (i.e., failed snap test).
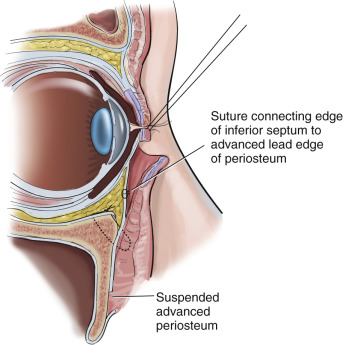
Once the periosteum has been resuspended, the orbital septum is opened and the postseptal fat is redraped over the infraorbital rim in an effort to blunt or eliminate the tear trough.
Rarely, and only in the most severe cases, is lower eyelid fat resected. The redundant periosteum, which now lies above the infraorbital rim, is used to cover the redraped fat and is sutured with a few 7-0 Vicryl interrupted sutures to the orbital septum while making sure that the Frost suture is retracting the lower lid superiorly. This redundant periosteum reinforces the orbital septum and adds volume to the lower lid ( Fig. 8.4 ).