The ethnic appearance of the Middle Eastern nose is defined by several unique visual features, particularly a high radix, wide overprojecting dorsum, and an amorphous hanging nasal tip. These external characteristics reflect distinct structural properties of the osseo-cartilaginous nasal framework and skin–soft tissue envelope in patients of Middle Eastern extraction. The goal, and the ultimate challenge, of rhinoplasty on Middle Eastern patients is to achieve balanced aesthetic refinement, while avoiding surgical westernization. Detailed understanding of the ethnic visual harmony in a Middle Eastern nose greatly assists in preserving native nasal-facial relationships during rhinoplasty on Middle Eastern patients. Esthetic alteration of a Middle Eastern nose follows a different set of goals and principles compared with rhinoplasties on white or other ethnic patients. This article highlights the inherent nasal features of the Middle Eastern nose and reviews pertinent concepts of rhinoplasty on Middle Eastern patients. Essential considerations in the process spanning the consultation and surgery are reviewed. Reliable operative techniques that achieve a successful aesthetic outcome are discussed in detail.
Demographics and scope
In the United States, the estimated size of the Middle Eastern diaspora ranges from 1.2 to 3.5 million people, depending on the census source. Most of this ethnic group (94%) reside in large metropolitan areas, particularly in the cities of Los Angeles, Detroit, and New York.
Patients of Middle Eastern extraction can trace their roots to 1 of the many countries in a vast geographic area of the Middle East. As ethnic and cultural borders of this part of the world have been blurred over the centuries by migration and intermixing of various populations, it is not surprising that people living in the Middle East and neighboring countries (Afghanistan, Pakistan, and India) have many of the nasal characteristics found in the Middle Eastern nose.
Because Middle Eastern extraction implies a wide range of ethnicities and religions, aesthetic needs and desires for rhinoplasty vary subtly between various geographic regions of the Middle East (and, by extension, within the diaspora presently living in the United States). For instance, people living outside the Arabian Peninsula and Gulf regions (Saudi Arabia, Kuwait, Qatar, UAE, Oman, and Iran) desire a greater change with rhinoplasty, in terms of dorsal reduction and tip projection.
The Middle Eastern nose
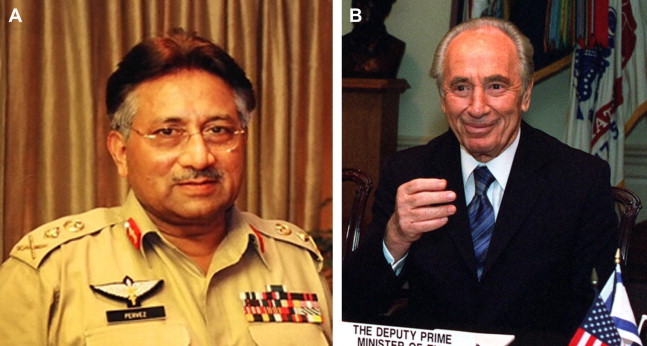
Several distinct surface features define the Middle Eastern nose ( Table 1 ). These features can be readily identified on photographs of people of Middle Eastern descent ( Fig. 1 ).
| Upper third | High radix, overprojecting bony dorsum, excessive dorsal width |
| Middle third | Widening of the osseous and cartilaginous vaults, straight of the brow-tip aesthetic line |
| Nasal tip | Amorphous hanging nasal tip, cephalically orientated lower lateral crura, weak medial crura, acute nasolabial configuration |
| Nostrils | Variable degree of alar flaring |
| SSTE | Thick oily skin, high density of pilosebaceous units, amorphous tip appearance, supratip fullness |
The upper two-thirds of the Middle Eastern nose is dominated by a high radix and a strong dorsum, with an associated dorsal hump. The dorsal hump is almost always accentuated by an under projected, hanging nasal tip, which creates the illusion of increased dorsal height. As a result, tip elevation is an important surgical maneuver in reducing this illusion and visually lowering the dorsum.
The cartilaginous framework of the lower one-third of the nose consists of weak lower lateral cartilages, resulting in varying degrees of nasal tip ptosis. The medial crura are typically thin and add minimal structural integrity toward nasal tip support. The lateral crura tend to have a cephalic orientation and contribute variably to supratip and supra-alar fullness. Overactive depressor septi nasi muscle and alar flaring can also be seen.
A thick overlying skin–soft tissue envelope (SSTE) covers the osseo-cartilaginous framework of the Middle Eastern nose. This property of the SSTE significantly influences the appearance of the lower one-third of the nose by blunting tip definition and adding fullness to the supratip and supra-alar regions. Around the nasal tip, numerous pilosebaceous units give the skin an oily texture and further contribute to increased skin thickness. In the postoperative period, pilosebaceous content of the SSTE promotes tissue scarring and pollybeak formation, caused by increased vascularity in the region.
The Middle Eastern nose
Several distinct surface features define the Middle Eastern nose ( Table 1 ). These features can be readily identified on photographs of people of Middle Eastern descent ( Fig. 1 ).
| Upper third | High radix, overprojecting bony dorsum, excessive dorsal width |
| Middle third | Widening of the osseous and cartilaginous vaults, straight of the brow-tip aesthetic line |
| Nasal tip | Amorphous hanging nasal tip, cephalically orientated lower lateral crura, weak medial crura, acute nasolabial configuration |
| Nostrils | Variable degree of alar flaring |
| SSTE | Thick oily skin, high density of pilosebaceous units, amorphous tip appearance, supratip fullness |
The upper two-thirds of the Middle Eastern nose is dominated by a high radix and a strong dorsum, with an associated dorsal hump. The dorsal hump is almost always accentuated by an under projected, hanging nasal tip, which creates the illusion of increased dorsal height. As a result, tip elevation is an important surgical maneuver in reducing this illusion and visually lowering the dorsum.
The cartilaginous framework of the lower one-third of the nose consists of weak lower lateral cartilages, resulting in varying degrees of nasal tip ptosis. The medial crura are typically thin and add minimal structural integrity toward nasal tip support. The lateral crura tend to have a cephalic orientation and contribute variably to supratip and supra-alar fullness. Overactive depressor septi nasi muscle and alar flaring can also be seen.
A thick overlying skin–soft tissue envelope (SSTE) covers the osseo-cartilaginous framework of the Middle Eastern nose. This property of the SSTE significantly influences the appearance of the lower one-third of the nose by blunting tip definition and adding fullness to the supratip and supra-alar regions. Around the nasal tip, numerous pilosebaceous units give the skin an oily texture and further contribute to increased skin thickness. In the postoperative period, pilosebaceous content of the SSTE promotes tissue scarring and pollybeak formation, caused by increased vascularity in the region.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


