This article discusses and presents options related to the cosmetic reduction of enlarged lips, primarily in ethnic populations. No formal study is performed. The author presents a literature review and discusses his personal 26-year experiences in lip surgery. When basic tenets are followed, cosmetic lip reduction is a predictable procedure with very little morbidity. Although lip augmentation is a popular cosmetic procedure, a certain percentage of the population desires smaller lips. Reduction cheiloplasty is a safe and predictable procedure that has been performed over a half century. This procedure is relatively simple and has a moderate learning curve. Cosmetic lip reduction is safe and effective, and has a high level of patient acceptance when certain diagnostic and treatment criteria are fulfilled.
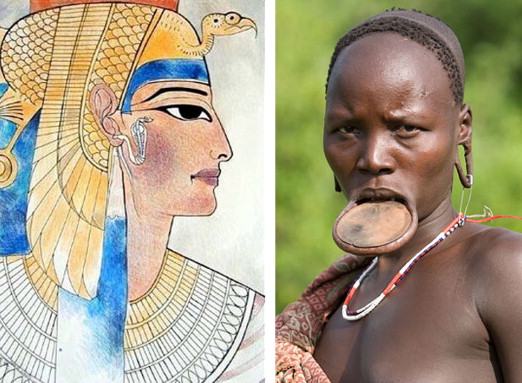
Lip enhancement has been a popular custom, especially in females, in most societies since the dawn of recorded history. Lip enhancement is the mainstay of the minimally invasive portion of most cosmetic facial surgery practices, but not all patients seeking cosmetic lip enhancement desire bigger lips. A certain percentage of the population seeks cosmetic consultation for lip reduction, and the cosmetic facial surgeon should be versed in this treatment option as well. In the author’s personal experience, most patients presenting for lip reduction are of African American heritage but the author has performed this procedure on patients from other ethnic groups, including multiple Caucasians ( Fig. 1 ).
Diagnosis and consultation
Macrocheilia defines a larger than normal lip. Various ethnic groups share the characteristic of larger lips including African American, Asian, and other groups ( Figs. 2 and 3 ). For the remainder of this article racial lip differences with larger lip anatomy are referred to as “ethnic” lips. This term would apply to racial groups that commonly have lips that are larger than the Caucasoid lip and more frequently seek cosmetic lip reduction.


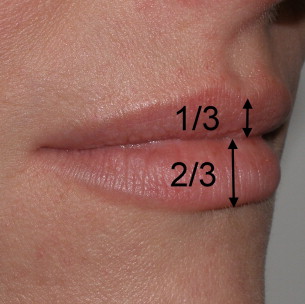
In the Caucasian patient the upper lip constitutes one-third of the total lip volume while the lower lip constitutes about two-thirds of the total lip volume, with a ratio of about 1:1.6 ( Fig. 4 ). African American lips are generally larger in all dimensions, and the upper and lower lip volumes are frequently nearly the same in many patients. Ethnic lips are also more protrusive, in part due to having more soft tissue mass. The normal chin and lip soft tissue thickness is approximately 12 mm in Caucasians and 15 mm in African Americans. Vermilion height norms vary in different ethnicities; for example, on average, African American males have 13.3-mm upper lips and 13.2-mm lower lips, and African American females have 13.6-mm upper lips and 13.8-mm lower lips. North American Caucasian vermilion height norms of upper and lower lip for males and females are 8.0 and 8.7 mm and 9.3 and 9.4 mm, respectively. In the normal situation there is a 0- to 3-mm intralabial gap between the lips in repose. Patients with larger intralabial space may not be good surgical candidates. The importance of ruling out dentofacial deformities as contributing factors to macrocheilia cannot be overstressed, and orthodontic, oral, and maxillofacial consultation and lateral cephalogram may be of assistance.
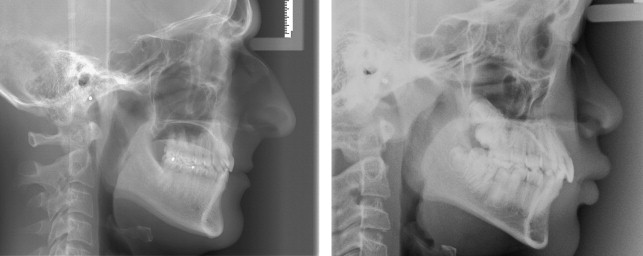
An additional contributing factor is fact that many African American patients exhibit a skeletal bimaxillary protrusion whereby the angulation of maxillary and mandibular alveolar bone and teeth protrude anteriorly, which influences the lip posture ( Fig. 5 ). If dentofacial abnormalities are not recognized, lip reduction may be contraindicated and may worsen the cosmetic deformity by overly reducing lip size and exposing the dentofacial deformity. Finally, microgenia can frequently accompany a bimaxillary protrusive profile, and the lack of chin prominence can make the lower lip appear larger ( Fig. 6 ).

A patient’s self image of his or her lips, like other body parts, is relative. Some ethnic groups have large lips and this is normal (and attractive) in that context. A subgroup of individuals in a given ethnic group may have bigger than normal lips (even for their ethnic type) and desire them smaller ( Fig. 7 ).

Unusually large lips (like any body part) aesthetically can make a person appear or feel unattractive. In addition, adverse stereotypical characterizations amplify this characteristic (especially a “dangling” lower lip) and associate it with being dumb or mentally slow (reminiscent of “Bubba” in the movie Forrest Gump). Function can also be affected by very large lips as it can make speaking or eating difficult in some cases, and promote drooling in the case of abnormal orbicularis oris muscle tone.
Other ethnic patients presenting for lip reduction do not have abnormally large lips for their race, but want to look more “international.” This desire falls into the same category as Asians altering their eyelids, African Americans straightening their hair, or Caucasians tanning their skin or getting lip filler. The author refers to this as the cosmetic paradox in that people with small features want big ones and people with big features want small ones. Beauty is truly in the eye of the beholder. Some people may say that “ethnic” patients have larger lips, whereas to “ethnic” patients Caucasians can be said to have small lips.
In a most eloquent dissertation on this subject Harold E. Pierce, a noted African American plastic surgeon from Howard University, states the following on the topic of race. “To the physician, as well as the public, there is confusion about the meaning of the word ‘race’ as applied to man. The biologist, however, who studies insects, plants, and other kinds of organisms about which there is on reason for emotional controversy, is not confused. To him a race is a collection, basically a group of individuals of both sexes definitely associated with a place of origin, habitually interbreeding and possessing a historical continuity in the reproduction of the general type. These individuals tend not only to look alike but to behave similarly. The concept of race includes differences in observable external characters, in behavior, in growth time and in other variables, all of which are genetically determined. In the long run, these variations serve to suit races to different environments or to different phases of a single environment. Near the Arctic Circle people are uniformly short; people native to areas of the greatest heat and sunlight tend to have dark skin and eye colors. The nose of an Arab would probably freeze were he to spend a day outdoors in Siberia, while flat faced Tungas are able to withstand extreme cold.”
Regardless of the desire, as for all cosmetic facial procedures, the surgeon must be certain that the patient is undergoing the procedure for the correct reasons and has reasonable expectations for the outcome.
Differential diagnosis
Macrocheilia can be due to ethnic variation, a result of dentofacial deformities (pseudomacrocheilia), from pathology such as lymphatic disorders or hemangiomas, and medical causes. Medical causes include Melkersson-Rosenthal syndrome, a rare neurologic disorder characterized by recurring facial paralysis, swelling of the face and lips (usually the upper lip), and the development of folds and furrows in the tongue. Ascher syndrome is a rare disease first described in 1920 by an ophthalmologist of the same name. The disease is characterized by a double upper lip, blepharochalasis, and nontoxic thyroid enlargement. These 2 medical entities often go undiagnosed, and the astute surgeon should always consider systemic disease as a contributing factor. In addition, some patients have lower lip ptosis due to orbicularis oris dysfunction or central nervous system problems, and orbicularis oris function should always be evaluated. Patients that cannot retract their lower lip or those with lip incompetence from poor muscle tone or other causes are not candidates for reduction cheiloplasty. Continual drooling may be a sign of poor muscle tone of the lower lip. These patients may benefit from a midline resection of lip and skin to shorten the width of the lower lip, which causes a sling effect in tightening the lip.
Differential diagnosis
Macrocheilia can be due to ethnic variation, a result of dentofacial deformities (pseudomacrocheilia), from pathology such as lymphatic disorders or hemangiomas, and medical causes. Medical causes include Melkersson-Rosenthal syndrome, a rare neurologic disorder characterized by recurring facial paralysis, swelling of the face and lips (usually the upper lip), and the development of folds and furrows in the tongue. Ascher syndrome is a rare disease first described in 1920 by an ophthalmologist of the same name. The disease is characterized by a double upper lip, blepharochalasis, and nontoxic thyroid enlargement. These 2 medical entities often go undiagnosed, and the astute surgeon should always consider systemic disease as a contributing factor. In addition, some patients have lower lip ptosis due to orbicularis oris dysfunction or central nervous system problems, and orbicularis oris function should always be evaluated. Patients that cannot retract their lower lip or those with lip incompetence from poor muscle tone or other causes are not candidates for reduction cheiloplasty. Continual drooling may be a sign of poor muscle tone of the lower lip. These patients may benefit from a midline resection of lip and skin to shorten the width of the lower lip, which causes a sling effect in tightening the lip.
Lip anatomy and histology
The lips serve many functions including eating, drinking, speaking, mimetic animation, kissing, and serving as a valve for the terminal oral airway.
The lips are among the most vascular structures on the face, and are supplied by the superior and inferior labial branches of the facial artery as it branches from the external carotid artery ( Fig. 8 ). The labial artery lies in the posterior one-third of the lip at about the incisor level ( Fig. 9 ). The depth of this artery is an important landmark to keep in mind, but fortunately is deep to most lip reduction procedures.
The anatomy of the lip is unique in that there is a triple transition from hair-bearing skin to vermilion tissue to oral mucosa. The hair-bearing skin terminates at the cutaneous/vermilion junction. The vermilion tissue consists of a very thin keratinized stratified squamous epithelium with extensive interdigitations with the underlying dermis ( Fig. 10 ).
The vermilion is devoid of hair follicles, sweat glands, and sebaceous glands (although they may be sparsely present). It is the lack of sebaceous glands that causes the vermilion to dry and crack and, hence, they must remain moistened with saliva. Anecdotally (because this statement cannot be scientifically qualified), people with naturally larger lips seem to moisten them with their tongue with much greater frequency than people with smaller lips.
The vermilion derives its color from the rich vascular plexus in the underlying dermis. This area is also highly sensitive due to its rich sensory innervation.
The thin keratinized stratified squamous epithelium of the exposed vermilion transitions into a thick, nonkeratinized, stratified squamous epithelium, and becomes the intraoral mucosa ( Fig. 11 ). Under this thicker epithelium lies a submucosa containing numerous accessory salivary glands including serous, mucous, and mixed seromucous glands. As the anterior vermilion surface meets the skin, hair follicles, sweat glands, and sebaceous glands are present ( Fig. 12 ).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


