Key Points
- ▪
Design the upper margin of the flap just below the lower border of the mandible to make the scar inconspicuous.
- ▪
Preoperative ultrasound is a valuable tool to evaluate the number of available lymph nodes and node location prior to flap harvest.
- ▪
The marginal mandibular nerve should be carefully identified and protected.
- ▪
Harvested lymph nodes are close to the facial vessels and careful dissection in the area will prevent injury.
- ▪
Harvest of the anterior belly of digastric muscle will ensure inclusion of the cutaneous perforator of the flap.
- ▪
Careful dissection and consideration of the submental artery near the submandibular gland will prevent inadvertent pedicle injury.
Introduction
Increasing options for vascularized lymph node (VLN) donor sites have allowed surgeons to make patient-specific decisions to individualize every case. A variety of donor site options are paramount to decision-making as certain patients may or may not be candidates for flap harvest from specific donor sites. The groin donor site continues to be the most popular and common source for vascularized lymph nodes. In the setting of lower extremity lymphedema, this option may not always be indicated due to increased fears of inducing morbidity in the unaffected extremity. The submental VLN flap represents a valuable option for a donor source of vascularized lymph nodes remote from the extremities.
The submental flap has been previously described in the setting of locoregional flap coverage of the head and neck region. This flap, based on the submental artery axis, was initially described in 1990 as a reliable cervical flap for a wide range of defects. Since its initial description, further cadaveric and clinical studies have found this flap versatile in the free or pedicled variety. In addition, refined anatomic considerations have allowed versatility in the design of this flap. Although many of the advancements of this flap help to decrease donor site morbidity and improve flap design, special consideration must be given for the VLN flap from this region. This chapter will detail the specific anatomy and surgical technique related to the successful execution of this vascularized lymph node flap.
Concepts
The flap, based on the submental artery axis, is similar in design and elevation as the traditional submental flap used in locoregional soft tissue coverage of the head and neck. Additional technical considerations must be given to the location, preservation, and perfusion of the lymph nodes in the region.
Regional Anatomy
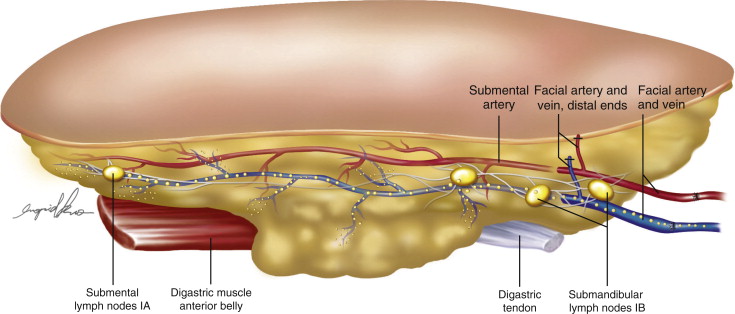
The key anatomic structures of the submental region are shown in Figure 16.1 . In the subplatysmal space, key structures can be found within the various layers of the investing layer of the cervical fascia. The main arterial sources to neck structures include branches of the external carotid system. The arterial supply to the submental VLN flap is based on the submental artery, which is a consistent branch of the facial artery. The facial artery can be found approximately 2.0–2.5 cm anterior to the mandibular angle at the level of the lower mandibular border. Approximately 0.5 cm below this point, the submental artery can be found originating as an anterior branch from the facial artery. The average arterial diameter at the origin is approximately 1.5–2.0 mm. The emergence of the submental artery is in close relation to the submandibular gland. In a majority of cases, the submental artery can be found between the lower border of the mandible and the submandibular gland. Occurring less frequently, the artery runs on the superficial surface of the gland or running between the lobes of the gland. Following the course past the gland, the artery travels on the superficial surface of the mylohyoid muscle, which separates the neck structures from the oral cavity. During the arterial course, the submental artery supplies various skin perforators through the platysma muscle. The distal aspect of the artery can have a variable course in relation to the anterior belly of the digastric muscle. In approximately 70% of patients, the distal submental artery travels deep to the digastric muscle, while the remaining travels superficial to the muscle. The different arterial variations are shown in Figure 16.2 . The venous system parallels that of the arterial supply with the submental vein draining into the anterior facial vein.
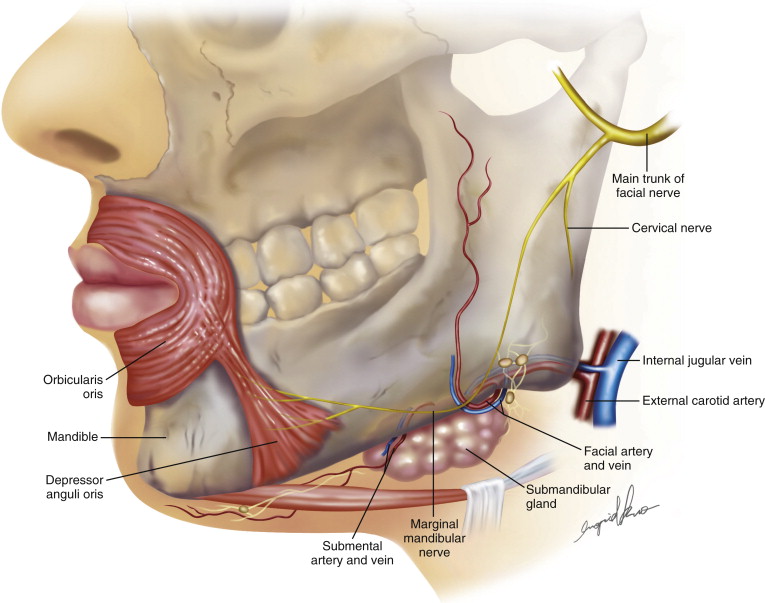
Special consideration is warranted for the location of the marginal mandibular branch of the facial nerve (MMN). An otherwise successful lymphedema-related surgical result will be overshadowed by the morbidity of injury to this important structure. Injury to the MMN manifests as weakness and/or inability to move the ipsilateral lower lip downward and laterally. Muscles responsible for this action are the depressor anguli oris (DAO) and depressor labii inferioris (DLI). Injury is apparent on animation of the face and asymmetry during smiling.
The MMN is one of the five major rami of the facial nerve. The clinically important location of the MMN is seen in the relationship of this nerve with the facial vessels, retromandibular vein, and the lower border of the mandible. Although early cadaveric studies suggest only a minority of patients have the MMN present below the lower border of the mandible, more recent anatomic studies suggest this location to be a more common clinical finding. Following the emergence of the MMN from the lower portion of the parotid gland, the nerve courses adjacent to the mandibular angle where variability in the branching pattern exists. In a cadaveric evaluation, Nelson and Gingrass found that the MMN had discrete, identifiable nerve branches to the DAO, DLI, and the mentalis. Branches to the mentalis and DLI consistently were located below the mandibular border. Anterior to the facial artery, the larger branch to the DAO was commonly located above the mandibular border and coursed deeply to innervate the muscle. Lower cervical branches were also identified at the lowest margins to innervate the platysma. The nerve branches are contained within a thin fascial layer superficial to the submandibular gland. In a clinical evaluation, Nason et al. found the MMN below the level of the mandibular border approximately 0–1.5 cm, but was more inferiorly displaced as much as 3 cm when the neck was extended.
Harvested vascularized lymph nodes included in the submental VLN flap are based on the level I nodes in the submental (IA) and submandibular (IB) regions. These lymph nodes are located in the subplatysmal plane atop the deep cervical musculature. The hyoid bone, the mandible, and the anterior belly of the digastric muscle designate the submental triangle. The anatomic landmarks of the submandibular group of lymph nodes are posterior to the submental region and continue from the digastric muscle posteriorly to the posterior aspect of the submandibular gland. Altogether, both groups comprise the level I lymph nodes and are in close proximity to the submental/facial artery system.
Patient Selection
Patient counseling prior to VLN transfer procedures will help to meet patient expectations in the postsurgical period. When specifically evaluating patients for submental VLN flap harvest, contour irregularities of the neck are the most likely potential morbidity in this region. In a heavy neck with significant preplatysmal fat, patient counseling on the possibility of asymmetries and contour irregularities must be discussed. In these cases, counseling on the possibility of contralateral neck procedures will help to balance the lower face and neck. In addition, previous surgery in the upper portion of the neck is a relative contraindication to flap harvest as scarring and reliability of lymph node inclusion is questionable. In addition to contour irregularities, iatrogenic injury to the MMN is a potential serious complication following harvest of the submental VLN flap. A thorough understanding of the course and relationship of this nerve to the vascular pedicle will minimize the occurrence of nerve injury (discussed above). Nevertheless, preoperative patient education to this potential complication is important during the consent process.
In the setting of lower extremity lymphedema, the submental VLN flap represents a remote VLN source that eliminates the chance of inducing lymphedema in the contralateral normal extremity. Harvest of level I lymph nodes in the neck has not been reported to cause iatrogenic lymphedema in the head and neck, and our clinical experience has supported this finding as well.
Preoperative Considerations
Lymphatic function testing in the preoperative setting is crucial to establishing the diagnosis and stratifying patients to the applicable procedure. Lymphoscintigraphy is the mainstay diagnostic test and is routinely used to assess lymphatic function. In regard to the submental donor site, preoperative lymphatic function testing is not necessary as lymph node harvest from this region will rarely result in head and neck lymphedema. Patient examination of the recipient site and donor site is an important consideration for this patient population. In advanced stage lymphedema patients, skin changes, cellulitic episodes, and the presence of open wounds may change the preferred recipient site to an alternate site unburdened by these infectious foci to eliminate the chance of complications related to infection. In cases of diffuse disease in the region of planned recipient sites, delayed reconstruction is performed. In the time interval prior to surgery, a strict protocol related to compression therapy and possibly antibiotics are necessary to eliminate the infectious burden.
General patient considerations prior to free tissue transfer are similar to other microsurgical procedures. A detailed patient history related to other medical conditions will allow for appropriate perioperative risk stratification. Cardiopulmonary considerations are typically the main determinants for microsurgical candidacy. Optimizing these systems will help to minimize the risks associated with long operative interventions and anesthesia-related morbidity.
Surgical Techniques
Flap Design
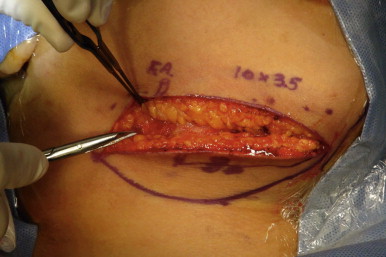
Design of the submental VLN flap begins with palpation and identification of the facial artery. The axis of the submental artery can be determined by the relationship of the artery and the lower border of the mandible. As mentioned above, the submental artery is a reliable branch of the facial artery and is located at approximately 0.5 cm below the lower edge of the mandible. In most cases, a skin island is needed to allow for recipient site closure. The elliptical skin paddle design is oriented along the long axis of the submental artery in order to capture perforating vessels to the skin. The superior half of the ellipse is limited to approximately 1 cm below the lower border of the mandible. Placing a higher incision may result in inevitable visibility of the scar on donor site closure. The lower half of the ellipse is then made and is adjusted based on neck skin laxity and the possibility of donor site closure. The limits of the skin paddle can extend to the midline or further depending on the needs of the surgeon. Figure 16.3 represents a standard skin paddle design measuring 10 × 3.5 cm. Narrower skin islands may be designed, which allow for decreased tension along the donor site closure and potentially a smaller scar along the lower border of the mandible.

Flap Harvest
![]() ( )
( )
Patient positioning for flap harvest includes prepping and draping of the neck as well as the lower face and corner of the mouth. Neck extension and rotation away from the intended side will aid in flap elevation and allow for assessment of facial mimetic muscles when dissection around the facial nerve occurs.
Following the appropriate surgical markings, the upper portion of the ellipse is incised first. The dissection is carried uniformly down to the level of the platysma ( Figure 16.4 ). Careful dissection then proceeds in the subplatysmal plane ( Figure 16.5 ) and identification of the facial artery and MMN first. Branches of the MMN are identified in close proximity to the facial artery as described above and careful dissection and manipulation will prevent inadvertent division and/or neuropraxia ( Figure 16.6 ). A nerve stimulator is a valuable tool used to identify all of the small branches that emerge from the MMN ( Figure 16.7 ). With neck extension, branches of the MMN can be seen as low as 1–2 cm below the lower mandibular border and must be carefully considered when dissecting in this region. Once the distal facial artery and MMN branches are isolated, flap elevation then proceeds from distal to proximal.
Related posts:
 An Introduction to Principles and Practice of Lymphedema Surgery
An Introduction to Principles and Practice of Lymphedema Surgery
 Clinical Evaluation of Lymphedema
Clinical Evaluation of Lymphedema
 Laboratory Study of Lymphedema
Laboratory Study of Lymphedema
 Recipient Site Selection in Vascularized Lymph Node Flap Transfer
Recipient Site Selection in Vascularized Lymph Node Flap Transfer
 Microsurgical Procedures: Minimizing Donor Site Morbidity Following Vascularized Lymph Node Transfer
Microsurgical Procedures: Minimizing Donor Site Morbidity Following Vascularized Lymph Node Transfer
 Future Perspectives in Lymphatic Microsurgery
Future Perspectives in Lymphatic Microsurgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


