Key Points
- ▪
Microsurgical lymph vessel transplantation is a reconstructive procedure to bypass the blocked lymphatic pathways in secondary lymphedema.
- ▪
Lymph vessel transplantation has proved its effect for over twenty years now.
- ▪
Long-term and stable results can be expected.
- ▪
Lymph vessel transplantation does not require supermicrosurgical skills.
- ▪
Donor site morbidity can be minimized by careful patient selection.
Introduction
Microsurgical lymphatic grafting was first described as ‘microsurgical lymph vessel transplantation’, although it is not a real transplantation, because blood supply is not provided during the operation. Lymph vessels are vascularized secondarily by the recipient site. In this chapter, we use the traditional term ‘lymph collector transplantation’ or ‘lymph vessel transplantation’ in addition to ‘lymphatic grafting’, because it has been used in the literature and on congresses.
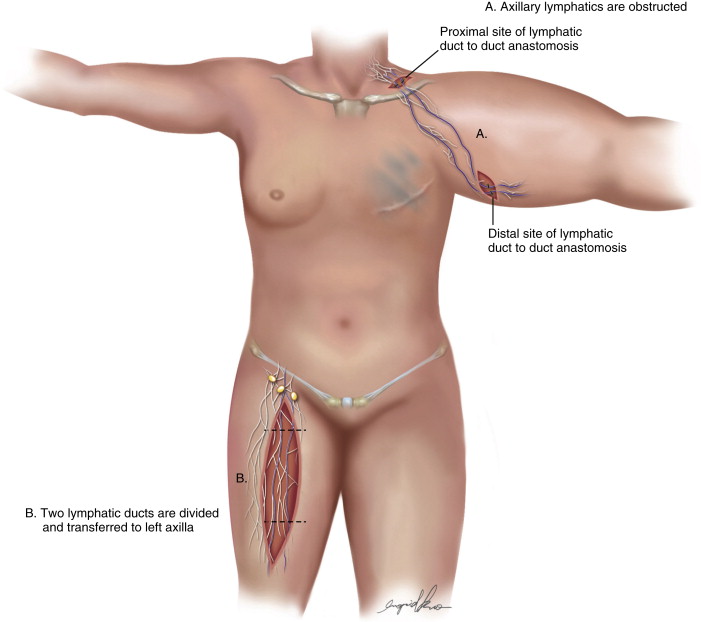
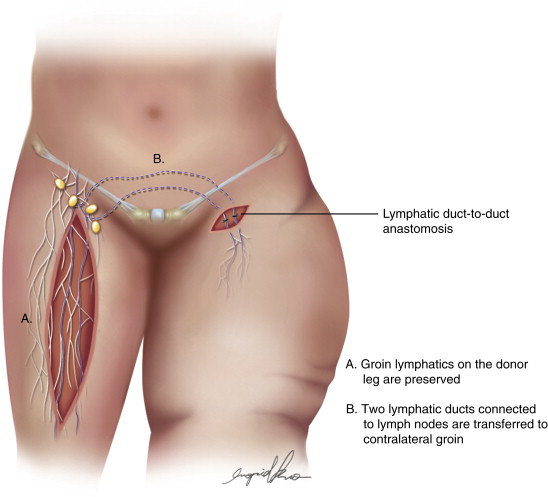
After many attempts to resolve the problem of chronic lymphedema, Professor Ruediger Baumeister came up with the idea of bypassing the regional blocked lymphatic system or lymph nodes depleted in the axilla ( Figure 21.1 ) and groin ( Figure 21.2 ) area with long lymphatic grafts. Other procedures were already known, but results were neither long lasting nor consistent. The operation was introduced in 1986 after animal research was successfully performed and after patency of the grafts had been demonstrated. Since that time, over 200 patients have been operated on and had thorough follow up. The results of these series have been previously published. This procedure is reproducible for every trained microsurgeon and adds another efficient strategy to the armamentarium of surgical procedures to treat lymphedema.
Concepts
Regional Anatomy
The Donor Site
The inner aspect of the thigh is especially suitable as a donor site for lymphatic grafting. In this region about 16–20 lymph collectors can be found in parallel. These vessels can sometimes be connected to each other by branching vessels, buiding a lymphatic net. The superficial lymphatic pathways can be found under the skin and above Scarpa’s fascia. But thicker and more reliable lymphatic vessels can be found under Scarpa’s fascia. Indocyanine green (ICG) injections cannot detect suitable vessels for lymphatic grafting because lymphatic vessels can only be seen 5–10 mm under the skin, but not under Scarpa’s fascia, nor in obese patients or patients with fat deposits in lymphedema.
When suitable lymphatic collectors cannot be found after some time of dissection, the collateral lymphatic trunks of the greater saphenous vein are always a good option because they are very consistent and their diameter is usually satisfactory. They can be harvested easily up until the knee area.
Anatomical findings of lymphatic vessels show many variations in humans. There are sometimes lymphatic vessels having quite a lot of branches. In other patients, lymph vessels do not branch over a long distance, which facilitates dissection of these vessels.
In obese patients, lymphatic vessels do have a three-dimensional course from superficial to deep and curve around bigger fat lobes, which may make dissection very tedious in these patients. In contrast, thin patients have lymphatic vessels that have a more parallel course and can easily be harvested, making these patients ideal candidates for performing the procedure.
In very rare cases, one cannot find suitable stained vessels, which are either too thin and are too easily damaged or only two to four vessels are stained by patent blue. In these circumstances, the anatomy shows a conditon of a weak lymphatic system and the surgeon is advised not to proceed as further dissection might damage overall lymphatic transport capacity. These patients are very vulnerable in getting donor site lymphedema after surgery.
There is a connection between the superficial to the deep lymphatic system about 10 cm above the knee near the adductor longus muscle insertion. This connection can be severed without risk. In some cases, lymphatic vessels have extensive branching making dissection over a longer distance not possible. If this is the case, then another lymph vessel shoud be evaluated. The diameter of the lymphatic vessels at the donor site range from 0.4 to 1.5 mm.
Recipient Lymphatic Vessels of the Inner Aspect of the Upper Arm ( Figure 21.1 )
Lymphatic trunks can consistently be found at the medial sulcus of the upper arm distal to the axilla. They can be found either above or below Scarpa’s fascia, but in chronic lymphedema, Scarpa’s fascia is not well defined in this area. If no vessels are present in this location or if they are too thin or too fibrotic, searching under the Scarpa’s fascia uncovers deep lymphatic vessels that are parallel to the blood vessels and nerves of the arm.The deep lymphatic vessels are always easily available and are a second option for recipient vessels.
Unfortunately, Patent Blue injections either in the hand or a small distance from the incision at the inner aspect of the arm are sometimes not helpful and do not show lymphatic vessels. Under magnification and careful dissection these vessels can nevertheless be identified because the course of the vessels is very consistent, and is strictly parallel to the neurovascular bundle of the upper arm.
Recipient Lymphatic Vessels of the Edematous Thigh ( Figure 21.2 )
Dissection and identification of lymphatic vessels is more difficult in the lower limb as compared to the upper arm because the course of the lymphatics is very often not parallel to the limb, but sometimes oblique. Also, neither Patent Blue or ICG injections in the foot nor distal to the recipient site leads to visualization of lymphatic vessels in the thigh. Small nerves can only be distinguished from lymphatics by good magnification and, when in doubt, by division of the structure and identification of lymphatic discharge of the vessel. Lymph nodes should not be severed during dissection as many lymphatics may enter one lymph node and functioning lymphatic pathways can be damaged easily.
The undisturbed anatomy in a healthy thigh is sometimes different to that in chronic lymphedema because collateral lymphatic pathways can be found in fibrotic tissue. This makes dissection in diseased tissues much more difficult in the recipient site compared to the donor site.
Anatomy of the Lymphatics in the Lateral Cervical Triangle
The lymphatic fat pad in the neck, known from surgery of the brachial plexus, is situated under the platysma on top of the brachial plexus. This tissue is very loose and contains many lymphatic vessels and also lymph nodes. Finding lymphatic structures can be quite difficult in this area as sometimes the lymph collectors are very small and fragile. Noninflamed and normal lymph nodes are very small, too. The directon of lymph flow is not obvious, as the orientation of the lymphatic vessels is rarely vertical as described and shown in anatomical textbooks. There are, however, always vertically oriented lymph vessels parallel to the internal jugular vein, but ligation of branching veins might complicate the dissection. In this region, it is sufficient to dissect 2–3 recipient vessels, which can be marked with vessel loops without tension. Injection in the face or behind the ear does not help to stain the desired vessels and may embarrass the patient as blue dye staining can remain for up to a year until the blue dye has vanished completely.
Patient Selection
Microsurgical lymphatic grafting is a procedure for localized obstruction in lymphatic drainage pathways. A bridge with a true bypass is built with the procedure. Therefore, it is not suitable for primary lymphedema, where there is generalized dysfunction of lymphatic transport. Patients with secondary lymphedema after axillary or groin dissection and subsequent radiation are ideal candidates; in rare situations, bridging of post-traumatic lesions and in facial and penile lymphedema have been reported.
The patient should present one healthy leg without compromised lymphatic transport. How should one estimate if a leg is healthy or not? It was shown by clinical practice that a thorough examination for pitting of the lower leg and ankle is sufficient. The patient should be asked about swelling of the ankle and lower leg: ‘Is there swelling in hot conditions or after standing or sitting to the point that you have problems in wearing your shoes?’ A minor pitting and swelling is normal and should not be called lymphedema. It is orthostatic edema. Of course, some may argue that hidden lymphedema might not show this way, but we think that a hidden lymphedema with no problems during summer and in situations where the leg was in dependent positioning for long periods of time is otherwise healthy. Lymphoscintigraphy might help to exclude some of those hidden lymphedemas. But false positive or negative results are also possible and this examination, involving the injection of radioactive colloids in or just below the skin, is not superior to a thorough medical history and examination. These considerations are very important for a successful operation, because the patient may have a concern for the possible iatrogenic donor site lymphedema in addition to the original devastating extremity lymphedema.
Related posts:
 An Introduction to Principles and Practice of Lymphedema Surgery
An Introduction to Principles and Practice of Lymphedema Surgery
 Clinical Evaluation of Lymphedema
Clinical Evaluation of Lymphedema
 Laboratory Study of Lymphedema
Laboratory Study of Lymphedema
 Recipient Site Selection in Vascularized Lymph Node Flap Transfer
Recipient Site Selection in Vascularized Lymph Node Flap Transfer
 Microsurgical Procedures: Minimizing Donor Site Morbidity Following Vascularized Lymph Node Transfer
Microsurgical Procedures: Minimizing Donor Site Morbidity Following Vascularized Lymph Node Transfer
 Future Perspectives in Lymphatic Microsurgery
Future Perspectives in Lymphatic Microsurgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


