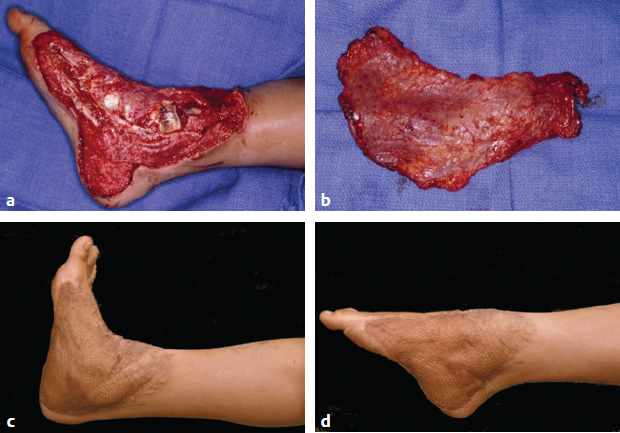
CHAPTER Complications in microsurgery have similarities with complications in any area of surgery; they can affect the outcome of the patient’s condition and discourage the surgeon and the medical team. Microsurgery is a technique, however, and no greater auras should be bestowed upon it. Thus all of the details and principles of surgery should be followed as they are for any surgical procedure. Perhaps one of the significant differences, though, in microsurgical complications is that there is a greater time investment and potential morbidity associated with the complications. Microsurgical complications can be grouped into very specific instances in which complications are more likely to occur (Box 15.1). Perhaps one of the greatest faults of any microsurgeon is that they perceive microsurgery as a hammer with every case presentation being a nail. A microsurgical reconstructive procedure may not be the most appropriate for a given patient or case scenario. Understanding that the anatomy, previous history of radiation, or comorbidities may significantly affect the overall outcome should play an important role in the decision-making regarding microsurgical reconstruction of any part of the body. Contraindications to reconstructive microsurgery are included in Box 15.2. Summary Box Complications Associated with Microsurgery • Complications of prolonged operations in microsurgery: – Myocardial infarction – Embolic event (deep venous thrombosis/pulmonary embolism) – Aspiration pneumonitis – Hypoxic brain injury – Death • Complications related to poor flap design: • Indications • Selection • Execution • Flap monitoring • Anticoagulants • Rehabilitation • Concomitant life-threatening injuries • Patient instability • Patients in hospice or receiving end-of-life care • Patients better served by an amputation or prosthesis • Patient noncompliance Every patient is unique. The reconstructive needs of individual patients demand a variety of reconstructive options and procedures. This is similar to other areas of medicine in which different patients are treated with different modalities to meet similar ends. As a physician treats hypertension, one patient may be prescribed one medication while another receives something different. Treatment in microsurgery is similar, with a given flap chosen specifically for a given patient to fit form and function. One of the challenges, however, is selecting patients who will not be subject to complications of the surgery. What may be more important for microsurgeons to understand are the factors that are not the absolute contraindications to performing microsurgery procedures but rather those for which the microsurgical procedure may be associated with a higher morbidity or even mortality in certain patients. Such conditions do not necessarily preclude free flap reconstruction, but these patients should be given thoughtful consideration and counseling about their potential increased risks of flap failure and potential complications.1–5 These conditions are included in Box 15.3. • Smoking • Obesity • Diabetes • History of hypercoagulability • Collagen vascular disorders • Use of medications that increase thromboembolic events (e.g., tamoxifen) • History of radiation • Steroid use/immunosuppression • Severe atherosclerotic disease • Renal disease • American Society of Anesthesiologists class (>3) Local or regional flaps may or may not prove better than the microsurgical free tissue transfer counterparts in some situations of complex reconstruction. The surgeon must evaluate what is best for the patient in terms of goals of the surgery, functional outcome, and, finally, aesthetic results. In a palliative surgery in which patient longevity is already determined by the cancer staging, local or regional flaps may actually suffice to provide the objectives of surgery that include wound closure and some element of functional recovery. Complex microsurgical procedures that prolong the patient’s time in the operating room may lead to increased blood loss, hypothermia, and morbidity and may not be indicated in these palliative circumstances.1,6,7 This does not mean that reconstructive microsurgery is not part of the algorithm of palliative surgery, but the surgeon must be aware of the increased risk of complications with microsurgery. Microsurgery is a technique used in the treatment of patients for various reconstructive procedures. Microsurgery should not be considered the only technique that patients are offered to best suit their needs. Complications of prolonged operations are addressed in the Summary Box. Every defect and every wound that is evaluated by the microsurgeon is unique in many ways. It is unique in the size, in the depth, in the location, in the composite structures that are involved, and in the functional loss that has ensued as a result of the preceding trauma or cancer resection. Flap design, therefore, is often rather innovative and must take into consideration all aspects of form and function. The goal is to restore normalcy. Over the last 30 years, the number of available donor sites has blossomed to allow the surgeon to choose the most appropriate compatible tissue that fulfills the goals of reconstruction yet minimizes the donor defects and optimizes patient satisfaction.8–11 Failures in design may arise from a number of different approaches to the reconstructive problem (see Summary Box). The design of the flap needs to meet the overreaching goals of the reconstructive surgery such that all required composite tissues are incorporated in the flap, the pedicle will reach the appropriate recipient vessels, the donor site morbidity is minimized, and flap surveillance is optimized11,12 (Figs. 15.1 and 15.2). Fig. 15.1 Flap design and selection. (a,b) A muscular flap with a skin graft, such as the free rectus shown in this patient, offers stable and well-vascularized coverage of the defect. (c,d) However, the bulk of this flap prevents the patient from wearing a shoe. Better options, such as a free fasciocutaneous or fascial flap with skin graft, not only provides similar successful coverage, but also results in a more functional final contour for the patient. Fig. 15.2 Flap design and selection. (a,b) This lower extremity wound was covered with a thin fascial flap and skin graft. (c,d) The outcome is stable coverage and a nicely contoured flap, which allows excellent range of motion. Furthermore, the flap bulk is reduced and allows the patient to wear a shoe. Microsurgical procedures rely on adequate donor and recipient vessels that are coapted without tension in a non-hostile environment. There are many principles involved in this aspect of reconstructive microsurgery. The recipient vessels should be nontraumatized, be easily accessible, and have significant caliber to provide inflow and outflow.13 Vessels identified within an area of inflammation or trauma or that is at risk of secondary contamination are inappropriate as recipient vessels.14 In 1992 Dr. Ian Taylor15 provided a total body overview of perforator anatomy where blood vessels arise from deeper main vessels to supply overlying angiosomes of skin. Each of those angiosomes or skin paddles could be transferred as a separate free tissue transfer based on one perforator.4 Microsurgeons, however, must use the most appropriate flap based on the most appropriate vessel that is perhaps based on the most appropriate perforator to achieve the most appropriate reconstructive result. Picking the right length of a pedicle is a “Goldilocks” phenomenon. If it is too long, it will kink. Kinking results in vascular obstruction and secondary clotting with flap compromise. If the vessel is too short and the anastomosis is performed under tension, the lumen size is diminished and flow dynamics change, which may lead to intraluminal clots and flap compromise.4 Therefore the “just right” pedicle length is imperative to secure adequate blood flow (Fig. 15.3). Identifying the best recipient artery and vein for the free tissue transfer is arguably one of the most important considerations in microsurgery. Recipient vessels must be easily accessible and in an easy site of surgery for the anastomosis. The vessels need to be accessible to the primary surgeon and the assistant for the anastomosis to be per formed flawlessly. Struggling in a poor recipient site with poor quality vessels will lead to poor outcomes! Fig. 15.3 Pedical position. This scalp replant demonstrates a nice resting curve of the vessels. The pedicle must lie in a smooth curve without too much tension, and similarly without too much redundancy, which may lead to kinking. There are many situations that may create a challenge to identifying the appropriate vessels for free tissue transfer. Such situations may include previous radiation, recurrent dissection, history of local infection, and location within the zone of trauma.1,14 Inflammation, fibrosis, and atherosclerosis change the native characteristics of the arteries especially. The arteries become more friable, are susceptible to intimal wall separation, and invite clot formation. Uninjured, disease-free vessels are devoid of any foreign material within the lumen. This is how the microsurgeon should want to see the lumen when performing the anastomosis. Lumen adulterants promote clot formation. With a little saline irrigation, the lumen should appear patent with white intima. Any haziness, red spots (clot fragments), webbing, free suture material, or gauze lint within the lumen needs to be removed before the anastomosis is complete or platelets will aggregate, form a clot, and result in vascular occlusion and, ultimately, flap compromise. Adventitial stripping is less important in clot formation and vessel preparation than suture placement. Thus loose ends of adventitia near the lumen edge may invert into the lumen during suturing. Adventitia within the lumen will be a nidus for platelet aggregation and clot formation. That does not mean the surgeon needs to strip a vessel 2 to 3 cm away from the anastomosis site. Other circumstances that lead to clot formation include intimal tears, retained long ends of tied sutures within the lumen, vascular clamp trauma, and injury to the vessel during vessel dissection. It is important for the surgeon to realize that both the surgeon and the assistant can cause intimal tears and vessel damage during early dissection. A dissection that is too aggressive may result in instrument trauma to the vessels. Similarly, having the assistant hold and provide some tension to vessel branch ends or suture ends at the anastomosis site may cause intimal tearing if too much tension is applied. The vessel end will need to be freshened again if a tied suture is pulled out or a tear is noticed at the suture site (Box 15.4). Whenever intimal damage is observed, it is prudent for the surgeon to cut the vessel back to an area proximal to the damaged vessel. This will set the stage for the best chances for patency.16,17 • Incomplete removal of adventitia • Intimal tears • Instrument trauma • Incomplete removal of existing clot in lumen • Existing trauma to the vessel wall All of the principles that apply to avoiding clot formation also apply to avoiding complications when performing the vascular anastomosis. In addition, a number of technical points should be emphasized that minimize the chance of platelet aggregation and thrombus formation18 (Table 15.1). The main caution with flap inset is the position of the vascular pedicle. Kinking of the artery or vein is a complication that leads to vascular occlusion and clot formation within the vessels. Although it is preferred to have a pedicle lie in a straight line after the anastomosis is complete, dramatic curves can be tolerated as long as the pedicle is not bent at the anastomosis site. The anastomosis is a point of weakness in the normal elastic properties of the blood vessel. A native vessel curves as a unit, whereas at the site of the anastomosis, the vessel caves in on the concave side of the bending vessel to form a 90-degree or smaller angle, which impedes flow, increases resistance and turbulence, and forms a thrombosis. The pedicle should be trimmed to an appropriate length so the vessels are not forced to kink when the flap is inset or when body position is altered postoperatively. Alternatively, the surgeon must be sure a long pedicle has a gentle curve that will not fold upon itself. If the pedicle is too long and the surgeon does not feel comfortable resecting some vessel and redoing the anastomosis, an easy fix is to place a piece of fat or muscle on the inner aspect of the curving vessel, preventing it from kinking at that site.19,20 Flaps that are closed under tension are also prone to vascular compromise as the pedicle is compressed. Postop erative swelling adds to the compression of the vessels. This complication is avoided by harvesting flaps slightly larger than a given defect. The opposite is true, however, for flaps inset into cavities, such as deep inferior epigastric perforator (DIEP) flaps in a skin-sparing mastectomy (Fig. 15.4). Table 15.1 Technical anastomotic suture tips to prevent patency failure
15
Microsurgery
Avoiding Unfavorable Results and Complications in Microsurgery
Indications
 Anesthesia-related risks:
Anesthesia-related risks:
 Nerve injury
Nerve injury
 Pressure sore development
Pressure sore development
 Postoperative delirium
Postoperative delirium
 Respiratory failure and ventilator dependence
Respiratory failure and ventilator dependence
 Bulk of flap
Bulk of flap
 Incomplete coverage of defect
Incomplete coverage of defect
 Vessel tension or kinking (leading to intraluminal clots and flap compromise)
Vessel tension or kinking (leading to intraluminal clots and flap compromise)
 Inset under tension
Inset under tension
 Design
Design
 Pedicle selection
Pedicle selection
 Flap elevation
Flap elevation
 Recipient vessel procurement
Recipient vessel procurement
 Flap inset
Flap inset
 Anastomosis
Anastomosis
 Clamp release
Clamp release
 Pedicle resting position
Pedicle resting position
 Final wound closure
Final wound closure
 Body positioning
Body positioning
Patient Selection
Execution
Design

Pedicle Selection
Recipient Vessel

Avoiding Clot Formation
Anastomosis
Flap Inset
 Donor site–related complications
Donor site–related complicationsTechnical tip | Rationale: clot producers |
Do not grasp the edge of the lumen. | Trauma exposes collagen. |
Remove all lumen debris. | Platelets will adhere. |
Do not use side branches as handles. | Intimal tears lead to collagen exposure. |
Use atraumatic dilators in the lumen. | Trauma causes intimal tears and collagen exposure. |
Clean suture of adherent blood. | Blood drags a clot into the lumen. |
Use the curve of the needle while suturing. | Lifting the needle may tear the lumen. |
Suture from inside out in lumens with intimal peel. | Intimal flaps will capture platelets or clots. |
Limit compression of vascular clamps. | Intimal damage leads to collagen exposure. |










