Microdermabrasion
Joyce Teng Ee Lim
M icrodermabrasion is a popular superficial skin resurfacing procedure performed by both physicians and nonphysicians. It is a simple, safe, and easy-to-perform cosmetic procedure with almost no downtime. This procedure is suitable for all ages. It is well tolerated with minimal side effects in darker racial ethnic groups (Fitzpatrick’s skin type IV through VI). Microdermabrasion is indicated for various cosmetic skin problems, including photodamage, 1,2 facial rejuvenation,3 cutaneous hyperpigmentation,4 acne,5 striae,6 and acne scars.7 Although little is known about the exact mechanism of action, there is evidence of dermal remodeling with minimal epidermal disruption. However, most of the studies involved small groups of patients. Despite the paucity of solid scientific data, most patients and some physicians are happy with microdermabrasion and perceived benefits from it.
Microdermabrasion Procedure
The first reported microdermabrasion was performed in Italy in 1985 by Marini and Lo Brutto, who reported both micro- and macroscopic improvement in the skin.2 They used a closed-loop negative pressure system that used microcrystals to abrade the skin. Since then, there have been many different machines using different types of crystals and different types of suction pressure systems. Initially, aluminum oxide crystals were used, but in later units, sodium chloride, sodium bicarbonate, or magnesium oxide crystals are used to minimize the risks from chronic inhaled aluminum oxide microcrystals. Some units do not use crystals; instead they use a firm diamond wand to microabrade the skin. Other units use positive instead of negative pressure systems.
During the procedure, the microcrystals strike the skin surface at an angle, and these are drawn across the surface of the skin by negative pressure airflow. Each crystal produces microtrauma to the skin, resulting in microabrasion. The used crystals and the skin debris are simultaneously aspirated by negative pressure from the skin surface into a container, and these are then discarded. The process is repeated as the handpiece is rapidly moved across the skin. Between each pass, a soft brush is used to wipe away excess crystals. The repetitive movement of the microcrystals across the skin causes intraepidermal injury to the skin, and this in turn causes a dermal response. Patients have to undergo several treatments to achieve the desired results. The time interval between treatments varies from 1 to 4 weeks, depending on the skin type and patient’s tolerance. Each session lasts from 20 to 30 minutes.
There are several factors that affect the depth and hence the efficacy of microdermabrasion Table 16-1. The pressure used, the flow rate of the crystals, the crystal size, and the angle at which the crystals hit the skin will determine the amount of microtrauma to the skin. The larger the crystal size, the greater will be the skin trauma, and the more acute the angle at which the crystals hit the skin, the greater will be the skin abrasion. Increasing the flow rate of crystals and the vacuum suction increases the depth of microdermabrasion. Other factors affecting the depth of microabrasion are the movement of the handpiece across the skin (the longer the dwell time, the greater the injury) and the number of passes.
Table 16-1 Factors affecting depth of microdermabrasion | |
|---|---|
|
There are three levels of microdermabrasion that can be achieved Table 16-2. Level 1 corresponds to a superficial epidermal abrasion. The handpiece is passed across the skin in one to two passes to achieve a cosmetic cleaning of the skin. This is usually done on the whole cosmetic unit. Level 2 is achieved when a higher vacuum pressure and more passes are used to get to the level of the papillary dermis. Here one can see minute pinpoint bleeding. This is usually
used for improving fine wrinkles, superficial scars, and striae. Level 3 will remove the whole epidermis, as well as a part of the dermis. This is used to improve striae, as well as wrinkles around the lips. Both levels two and three are associated with a higher incidence of side effects and should be performed by the physician. Level 2 and 3 microdermabrasion should be used with extreme care and caution in darker skin types to avoid complications, including hyperpigmentation, hypopigmentation, and scarring Table 16-3.
used for improving fine wrinkles, superficial scars, and striae. Level 3 will remove the whole epidermis, as well as a part of the dermis. This is used to improve striae, as well as wrinkles around the lips. Both levels two and three are associated with a higher incidence of side effects and should be performed by the physician. Level 2 and 3 microdermabrasion should be used with extreme care and caution in darker skin types to avoid complications, including hyperpigmentation, hypopigmentation, and scarring Table 16-3.
Table 16-2 Depth of microdermabrasion | |||
|---|---|---|---|
|
Indications
Microdermabrasion is used to treat a variety of skin problems, including photodamage,1,2 facial rejuvenation,3 cutaneous hyperpigmentation,4 acne,5 striae,6 and acne scars.7
Table 16-3 Side effects of microdermabrasion | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
Photodamage
Microdermabrasion can improve photodamaged skin, especially those with Glogau photoaging class I and II. Tan et al.1 analyzed the effect of microdermabrasion on skin surface roughness, topography, elasticity, stiffness, compliance, temperature, sebum content, and histology. Ten patients, Fitzpatrick skin types I through III, with photodamage (Glogau scale II and III) were treated at weekly intervals for five to six treatments using the Parisian Peel (Aesthetic Technologies Inc., Colorado Springs, CO). Nine patients had at least five treatments. The face received four passes at a vacuum pressure of 30 mm Hg while the periorbital skin received two passes at a pressure of 15 mm Hg. Improvement was seen in seven patients, six had mild improvement, and one had moderate improvement. The remaining three with no improvement had Glogau photoaging class III. Immediately after the procedure, there was a temporary increase in skin roughness, corresponding to the superficial abrasion, and in skin temperature, consistent with increased blood flow. Surface sebum decreased immediately after the procedure, but this effect did not persist between treatments. Skin stiffness decreased and skin compliance improved where microdermabrasion was done on the cheeks. Histologic studies did not show any change in collagen or elastic content. The epidermis showed some orthokeratosis and reduced rete ridge pattern. The upper reticular dermis showed a perivascular mononuclear cell infiltrate and vascular ectasia.
Microdermabrasion as shown by Shim et al.2 significantly improved skin roughness/textural irregularities, mottled pigmentation, and overall skin complexion in photodamaged skin. It did not significantly improve fine skin wrinkles.
Facial rejuvenation
Microdermabrasion can improve facial aging and is often used as part of a program for facial rejuvenation. Hernandez-Perez and Ibiett3 treated seven women, six with Glogau’s photoaging class II and one with Glogau’s photoaging class III. All had five microdermabrasion sessions, each having three passes per session, repeated at weekly intervals. At the start of treatment, all patients had oily skin, dilated pores, fine wrinkles, and thick skin in varying severity. There were improvements in all clinical variables after each weekly session, and the improvements were considered good to excellent. Patients also reported improvement in their self-esteem. Biopsies taken from these women before and after the fifth microdermabrasion sessions showed histopathological improvements. There was mild to moderate improvement in dermal elastosis and mild improvement in dermal inflammation, edema, and telangiectasias.
Hyperpigmentation
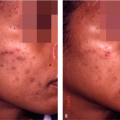
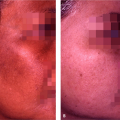
Microdermabrasion can improve the mottled pigmentation associated with photodamaged skin.2 Cotellessa et al.4 treated 20 female patients with multiple hyperpigmented macules of the face. Eight patients had complete clearance of the pigmentation after four to eight treatments, whereas ten patients had partial clearance after eight treatments. Two patients did not respond after eight treatments. When 15% trichloroacetic acid peels were combined with microdermabrasion treatments, fewer treatments (four to six) were needed to clear or partially clear the pigmentation Fig. 16-1 and Fig. 16-2). Microdermabrasion is often
used to treat melasma in conjunction with topical treatments. It probably works by enhancing the penetration of topical agents for melasma Fig. 16-2A,B




used to treat melasma in conjunction with topical treatments. It probably works by enhancing the penetration of topical agents for melasma Fig. 16-2A,B
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
