Nasal reconstruction remains a significant surgical challenge. The melolabial flap and its multiple variations relies on the robust vascularity and abundant subcutaneous fat of the melolabial fold, to transfer skin and soft tissue to the lower one-third of the nose, the nasal sidewall or as a replacement for nasal lining while hiding the donor scar in the melolabial crease. This content discusses pertinent cutaneous anatomy, patient selection, preparation and education, flap design, surgical techniques and post-operative considerations to enable the surgeon to achieve a reconstruction result that closely approximates the pre-injury state while producing limited donor site deformity.
Nasal defects, particularly those created by Mohs surgery to eradicate locally invasive skin carcinoma, can leave the patient with a deformity of significant magnitude. The challenge for the reconstructive surgeon, as in all cases, is to recreate the patient’s normal anatomy as accurately and naturally as possible with a minimum of additional noticeable scar. Regardless of the circumstance that leads to the nasal deformity, the reconstructive options selected, closely related to the skill and artistry of the surgeon, most often dictate the aesthetic and functional outcome of the reconstructive effort. Due to the critical function of the nose, nasal breathing must be maintained or in some cases improved during reconstruction. This functional challenge, in addition to the importance of nasal appearance to one’s sense of identity and attractiveness, makes nasal reconstruction a particular challenge.
Defects of the nose that are too large to close using local nasal flaps, are not appropriately repaired with a skin graft or are unfavorable for healing by secondary intention, regional flaps present an important, available source of vascularized soft tissue for reconstruction. Although there are several important regional flaps available for nasal reconstruction, the melolabial flap is one of the workhorse flaps used by the nasal reconstructive surgeon. This article reviews the anatomy of the melolabial fold; the various designs, applications, advantages, and disadvantages of the melolabial flap; preoperative considerations, patient education, and photodocumentation; the types and size of nasal defects best addressed with these flaps; the technical aspects of surgical execution; and the postoperative measures required to obtain an optimal, aesthetic, and functional result.
Anatomy of the melolabial crease and fold
The melolabial crease is an important facial landmark, which grossly distinguishes the cheek from the lips. It is also recognized as the nasolabial crease because it provides a distinction between the caudal aspect of the nose and the cheek. However, the preferred terminology is the melolabial crease as it best describes this anatomic feature. Understanding the anatomy of the melolabial crease and corresponding fold is essential not only for fashioning the melolabial flap but also for a comprehensive appreciation of the changes that take place in the aging face. The anatomy of this crease and fold have been described extensively in prior publications; this article delineates the gross anatomy, histology, and pertinent vascular and neural anatomy of the melolabial region as they each are related to the creation of melolabial flaps.
Gross Anatomy
The mimetic muscles of the face are surrounded by a layer of fascia known as the superficial musculoaponeurotic system (SMAS). This fascial layer continues as the platysma in the neck and as the frontalis muscle in the forehead, eventually becoming the galea aponeurotica of the scalp. Overlying the temporal region, this fascia continues as the temporoparietal fascia. The SMAS overlies the parotid gland, superficial to the parotidomasseteric fascia. In this region, studies have shown the SMAS to be thick and fibrous. As the SMAS continues medially toward the melolabial fold, its fibrous connective tissue becomes progressively thinner because it envelops the mimetic muscles, including the zygomaticus major, zygomaticus minor, orbicularis oris, levator labii superioris, depressor labii inferioris, levator anguli oris, and depressor anguli oris. All these muscles surround the melolabial fold and send out vertically oriented fibrous septa to the dermal layer of the skin. This construct allows the face to express a broad spectrum of emotions, based on the relative contractions and actions of these mimetic muscles.
At the junction of the cheek and lip, there is a dense concentration of the fibrous mimetic muscular decussations. This consolidated area of fibrous extensions results in the melolabial crease. There is a thicker layer of subcutaneous fat lateral to the melolabial crease that facilitates a smooth gliding motion of the mimetic muscles in relation to the skin. These fibrous extensions must traverse this fat layer, and thus, movement of the facial muscles moves both the skin and the thick fat layer below it. Medial to the melolabial crease, however, there is virtually no subcutaneous fat, and some studies suggest that the orbicularis oris fibers attach directly to the dermis in this region. The juxtaposition of the thick subcutaneous fat layer lateral to the crease compared with the subcutaneous tissues overlying the orbicularis oris, which is devoid of fat, creates what is clinically recognized as the melolabial fold. This lateral fat layer is clinically important because it provides adequate bulk and vascularity to the melolabial flap.
Histology
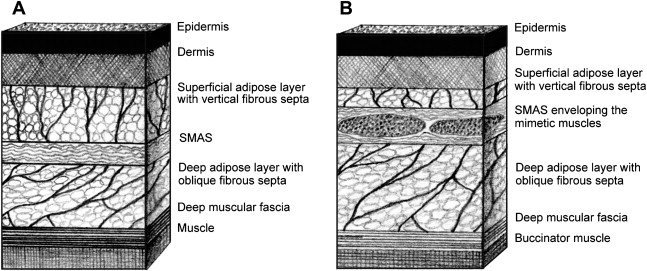
Evaluation of the microscopic anatomy of the melolabial area reinforces the findings of gross dissection. The following structures are encountered in sequence as the analysis moves from superficial to deep layers: epidermis, dermis, superficial adipose layer with vertically oriented fibrous septa, SMAS (a laminar layer of connective tissue), deep adipose layer with obliquely oriented fibrous septa, and deep (muscular) fascia ( Fig. 1 ). While moving from the lateral cheek to the melolabial crease, the superficial adipose layer and SMAS thin, whereas the deep adipose layer thickens. Additionally, the SMAS envelops the mimetic muscle of the medial face. Thus, the vertically oriented fibrous septa found within the superficial adipose layer connect the SMAS to the dermis and transmit muscular movements to the skin. This transmission allows the facial skin to move and express emotions.