Medium-Depth Chemical Peels and Deep Chemical Peels
Rashmi Sarkar
Chemical peeling is a cosmetic procedure that involves the application of one or more exfoliating agents to the skin to wound the epidermis and dermis in a controlled fashion. The goal is to cause subsequent regeneration of portions of epidermis or dermis with long-lasting improvement in the aesthetic quality and appearance of the skin. The use of chemical peels for beautifying the skin dates back to ancient Egypt when sour milk (lactic acid) was used by Cleopatra to produce a more cosmetically elegant appearance of the skin.1 Over the years, dermatologists pioneered chemical peeling for therapeutic uses.1 2,3,4,5, and 6 In 1882, Unna introduced the use of salicylic acid, resorcinol, phenol, and trichloroacetic acid (TCA) as skin peels, and in 1952, Mackee published his work on phenol peels for acne scarring.2 But it was Stegman’s benchmark work in the early 1980s, on the histological changes of wound injury after chemical peeling, that provided a scientific basis for the classification of chemical peels and paved the way for their application in a controlled and scientific way on the human skin.3 This further influenced the development of medium depth and chemical peels.4,5
A medium-depth chemical peel refers to a peeling agent or a combination of agents that cause destruction of the epidermis and the papillary dermis and may extend to the upper reticular dermis.6 Deep chemical peels produce destruction to the deeper reticular dermis and also induce new collagen and ground substance production. Rubin has provided a simplified working classification based on the depth of the wound created by the chemical peeling agent Table 18-1.7 The medium-depth peels, according to his classification, are glycolic acid 70% (applied for a variable time, 3 to 30 minutes); TCA 35% to 50%; and combinations of 35% TCA, with either CO2 snow, Jessner’s solution, or 70% glycolic acid, as well as unoccluded 88% phenol. Eighty-eight percent phenol and Baker-Gordon phenol formula are used as deep chemical peels. The most suitable candidates for medium and deep chemical peels are those who have fair (type I or II) photodamaged skin with actinic elastosis, fine facial wrinkles, and extensive actinic keratoses.8 Medium-depth peels are used sparingly in darker-skinned individuals because of a greater risk of postinflammatory hyperpigmentation. Darker-skinned patients are unsuitable candidates for a deep chemical peel because of more pronounced complications, namely hypopigmentation, hyperpigmentation, uneven skin pigmentation, and scarring, which can cause great emotional distress.9 As the risks of deep chemical peels far outweigh the advantages, they are best avoided in darker-skinned individuals.
Medium-Depth Chemical Peels
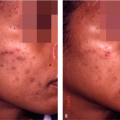
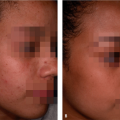
Medium-depth chemical peels are done by some experienced dermatologists in darker-skinned patients for diffuse or multiple actinic keratoses; pigmentary dyschromias, especially blotchy hyperpigmentation; postinflammatory hyperpigmentation or recalcitrant melasma that have not responded well to medical treatment or repeated light chemical peeling; fine to medium rhytides; and superficial acne scars (Table 18-2). Although TCA 35% to 50%, glycolic acid 70% (applied for 3 to 30 minutes), and phenol 88% can be used as solo medium-depth peeling agents, the new popular trend is to combine two less potent peels to minimize the risks by first penetrating the epidermis with a superficial peeling agent, which allows a more even and complete penetration of the medium-depth peel, 35% TCA.10,11
Each dermatologist must standardize the peeling procedure in the way he or she primes, cleans, and degreases the patient’s skin and applies the chemical agent to the skin to achieve optimum results. The factors affecting the depth of the peel are the peeling agent; the concentration of the peel; the number of coats applied; the technique of application; the method of priming, cleaning and degreasing the skin; the skin type; the anatomic site of the lesion; and the duration of contact with the agent.12 Before the procedure, it is important to perform a prepeel evaluation of the patient. A detailed history—including prior history
of abnormal scarring, use of medications such as isotretinoin and photosensitizing drugs, occupation, smoking, sun exposure, immunosuppression, and a history of herpes simplex—must be elicited. Cutaneous examination would include assessing the quality, texture, and tone of the skin; the skin type; and the amount of photodamage present. One may also make a reasonable assessment of the patient’s expectations. The contraindications to medium and deep chemical peels are abnormal scarring, active herpes simplex or bacterial infections, immunosuppression, uncooperative patient, unrealistic expectations, open cuts or scratches on the face, history of delayed wound healing, any facial surgery within 3 months, a mentally unstable patient, and use of isotretinoin therapy within the last 6 months.7,9,12,13 Some authors recommend using acyclovir orally in all patients, from the start of the procedure for the next 2 weeks.12
of abnormal scarring, use of medications such as isotretinoin and photosensitizing drugs, occupation, smoking, sun exposure, immunosuppression, and a history of herpes simplex—must be elicited. Cutaneous examination would include assessing the quality, texture, and tone of the skin; the skin type; and the amount of photodamage present. One may also make a reasonable assessment of the patient’s expectations. The contraindications to medium and deep chemical peels are abnormal scarring, active herpes simplex or bacterial infections, immunosuppression, uncooperative patient, unrealistic expectations, open cuts or scratches on the face, history of delayed wound healing, any facial surgery within 3 months, a mentally unstable patient, and use of isotretinoin therapy within the last 6 months.7,9,12,13 Some authors recommend using acyclovir orally in all patients, from the start of the procedure for the next 2 weeks.12
Table 18-1 Classification of medium-depth and deep chemical peeling agents | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
Trichloroacetic acid
TCA (35%–50%) is considered to be the gold standard for chemical peeling agents because of its long history of usage, stability, low cost, and versatility.8,13 As compared with phenol peels, it does not require lengthy consultation with the patient, has few medical contraindications, has no systemic toxicity, and, as pain is less severe and of a shorter duration, anaesthesia—whether intramuscular, intravenous, or general—is optional.14
It is usually prepared by a weight-to-volume aqueous solution. One hundred percent TCA is available in crystal form, which is colorless and ready to be diluted with water. To prepare a 30% concentration, 30 g of TCA crystals are added to distilled water to get a total volume of 100 mL. Similarly, various other concentrations can be prepared. The solution must be prepared fresh every 6 months. As the crystals are hygroscopic, they have to be stored in tightly capped, acid-resistant plastic or glass bottles. Once prepared, the TCA solution is light sensitive and therefore has to be stored in amber-colored bottles. To avoid contamination, the solution should be poured from a master bottle into a separate container for each peel procedure.
Table 18-2 Indications for medium-depth and deep chemical peeling | |||
|---|---|---|---|
|
The mechanism of action of TCA in chemical peeling is that it precipitates epidermal proteins and causes dermal inflammation, necrosis, and sloughing. This is visualized as white frosting on the skin surface. The white frost signifies the completion of the reaction and may also correlate with the depth of peel. Because of the increased risk of complications in darker-skinned patients in the form of postinflammatory hyperpigmentation, hypopigmentation, and scarring, strengths above 50% have been discontinued.12,13 In the author’s experience, a good prepeel preparation with a sole priming agent or their combination followed by a good cleansing and degreasing of the face can be effective for carrying out 35% TCA peels in selected and well-motivated darker-skinned patients only. Currently, the popular trend in medium-depth peeling is to combine two less potent agents to minimize complications of a single medium-depth peel. Penetration of the epidermis is achieved with a superficial peeling agent, and this is followed with 35% TCA application.14 These are done as single procedures with a healing time of 7 to 10 days.
Solid CO2 and 35% trichloroacetic acid
Brody first developed the combination of solid CO2 and 35% TCA as a medium-depth combination peel in 1986.4 Acetone is used to degrease the skin. A hand-sized piece of solid CO2 is dipped in a 3:1 solution of acetone and alcohol and then applied to the affected areas with varying degrees of pressure. The preliminary freezing with solid
CO2 helps to break the epidermal barrier and allows a more even and complete penetration of the deeper 35% TCA.15 To the edges of the depressed scars and to larger actinic keratoses, hard pressure can be applied for a better clinical result. Erythema with microvesiculation is the end point. After wiping the skin with acetone, 35% TCA is applied with cotton applicators to complete the procedure. This is considered a potent combination peel.
CO2 helps to break the epidermal barrier and allows a more even and complete penetration of the deeper 35% TCA.15 To the edges of the depressed scars and to larger actinic keratoses, hard pressure can be applied for a better clinical result. Erythema with microvesiculation is the end point. After wiping the skin with acetone, 35% TCA is applied with cotton applicators to complete the procedure. This is considered a potent combination peel.
Jessner’s solution and 35% trichloroacetic acid
Monheit introduced the use of Jessner’s solution before the application of 35% TCA in 1989.5 The Jessner’s solution acted as a keratolytic and destroyed the epidermal barrier to allow a deeper and more even penetration of 35% TCA. Although most of the studies evaluating the efficacy of medium-depth peels as a therapeutic modality are from the West, a combination of Jessner’s solution followed by the application of 35% TCA was found to be an effective and safe way of treating acne scars, even in patients of dark complexion, in an open study of 15 Iraqi patients.10 In the opinion of Al-Waiz et al., this medium-depth peel is one of the most effective simple and safe combinations if performed carefully by an experienced dermatologist in only selected patients, even in India. The procedure is described as below.
Prepeel evaluation
The initial prepeel consultation is important for patient selection and to gauge the patient’s expectations. A pertinent history is taken, and contraindications are ruled out. The procedure is explained realistically and in detail to the patient, including the postoperative erythema, swelling, and peeling that would keep the patient homebound for 7 to 10 days. Many patients are able to return to work in 7 days. The patient is also informed about potential complications. Strict sun avoidance is advised for at least 14 days. A written consent is obtained from the patient, and prepeel photographs are also taken.
Prepeel preparation
Preparing the skin for a chemical peel, or priming, is an important constituent in chemical peeling.16 A single prepeeling agent or a combination of agents can be used for at least 2 to 6 weeks before chemical peeling, and they can be continued as a maintenance regime after the peels. Prepeel or adjunct topical agents reduce the seborrhea and thin the epidermis, allow a more rapid penetration of the peel, accelerate re-epithelization and wound healing, decrease the risk of postinflammatory hyperpigmentation because of the bleaching effect caused by the dispersion of melanin granules, and enforce the concept of maintenance regime.13,16




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
