Introduction
Commonly, mastopexy is understood to be synonymous with “breast lift.” Among plastic surgeons, a mastopexy has been traditionally understood to mean a skin tightening procedure, certainly for a skin-only mastopexy. However, the goal of a mastopexy is improvement in the shape of the breast, not simply tightening of its elastic envelope. In ptotic breasts, the lower pole is usually reduced (i.e., parenchymal resection) to achieve an aesthetic lower pole and avoid a “mastopexy wrecking bulge.”
Many plastic surgeons use the term vertical scar mastopexy. However, the scar is not always vertical. The scar is frequently modified to a short inverted T. The scar may resemble a Wise pattern scar, but the parenchymal treatment is much different. Accordingly, vertical mastopexy is best labeled “vertical,” referring to the vertical midline parenchymal resection of the lower pole, not the scar.
Indications and Contraindications
For the woman who lifts her breasts by the cups of her hands and says, “This is what I want,” a vertical augmentation/mastopexy is likely to be most satisfactory, in accordance with the minus-plus principle. A patient who says, “I like my size, but just want it up here,” should be advised that such a result is impossible with a mastopexy alone. Breast remodeling is needed—more on top, less on the bottom—and this effect can be accomplished only by simultaneously inserting implants.
Measurements confirm that the inframammary fold (IMF) level moves up after a vertical mammaplasty. Both vertical and inverted-T techniques can elevate the lower pole. However, only the vertical method elevates the IMF. When a Wise pattern and inferior pedicle are used, the IMF remains fixed at the base of the pedicle.
An underappreciated benefit of elevation of the IMF and lower breast pole is the appearance of a longer torso. With the emphasis on fitness in our culture, and the frequent display of the abdomen, this anatomic area takes on greater importance. However, upward mobilization of the superior border of the breast is more challenging. Breast implants are needed to substantially boost breast projection and upper pole projection, , , providing the illusion of breast mound elevation. The author inserts breast implants in more than 70% of patients undergoing a mastopexy. A vertical mammaplasty, with a medial, superior, or superomedial pedicle is now used exclusively by a growing number of plastic surgeons.
Although smoking is never advisable, a smoking history is not an absolute contraindication to surgery. The vertical approach is more robust than the inverted-T, inferior pedicle technique because the keel-shaped lower pole parenchymal resection is not accompanied by skin undermining. Nipple–areola perfusion is optimized by preserving medial and deep vascular pedicles. Nevertheless, patients are instructed not to smoke during the perioperative period to reduce the risk of delayed healing, suboptimal scars, and nipple–areola tissue loss.
Preoperative Evaluation and Special Considerations
The mastopexy candidate presents with breast ptosis. The nipple position is evaluated. Patients are informed that implants provide minimal, if any, nipple elevation. Breast implants are not a substitute for a mastopexy. Implants do not adequately “take up the slack.”
The areola size is a consideration. Women with large areolae may wish to have them reduced, making the periareolar scar a favorable trade off. Existing breast asymmetry is the rule, not the exception. Patients are informed of their existing asymmetry and the fact that perfect symmetry is not realistic.
Patients may have had a previous augmentation. This is the time to discuss whether to replace the implants. Considerations include the desired size and the number of years the implants have been in place.
Patients who have had a previous breast lift may be candidates for secondary mastopexy. The original method used does not matter. Obtaining the original operative report is generally unnecessary. The author makes no attempt to replicate the original resection pattern. However, the surgeon must be especially careful regarding blood supply, often including the (de-epithelialized) superior areola hemi-circumference.
Many women who have had a previous Wise pattern mastopexy or reduction already have over-elevated nipples that do not require any additional elevation. Existing nipple overelevation may be improved or corrected by the elevating effect of the vertical lift on the breast mound. The challenge is to site the nipple as low as possible without leaving a scar superior to the nipple–areola.
Vertical Method
The vertical technique lengthens the lower pole distance (the length along the lateral curve from the plane of maximum postoperative breast projection to the posterior breast margin ), a measure of breast constriction, by converting an elliptical defect to a vertical straight-line closure. , , The lower pole is elevated, and the length dividend increases projection. , ,
Simultaneous Breast Implants
Some surgeons think that a mastopexy and breast implant work at cross purposes because a mastopexy tightens the skin envelope whereas a breast implant stretches it. The procedures are in fact synergistic when a vertical method is used. Implants make mastopexy easier to perform. There is less gathering of tissue in the lower pole. An inverted-T modification is less often required because the implant fills out the lower pole.
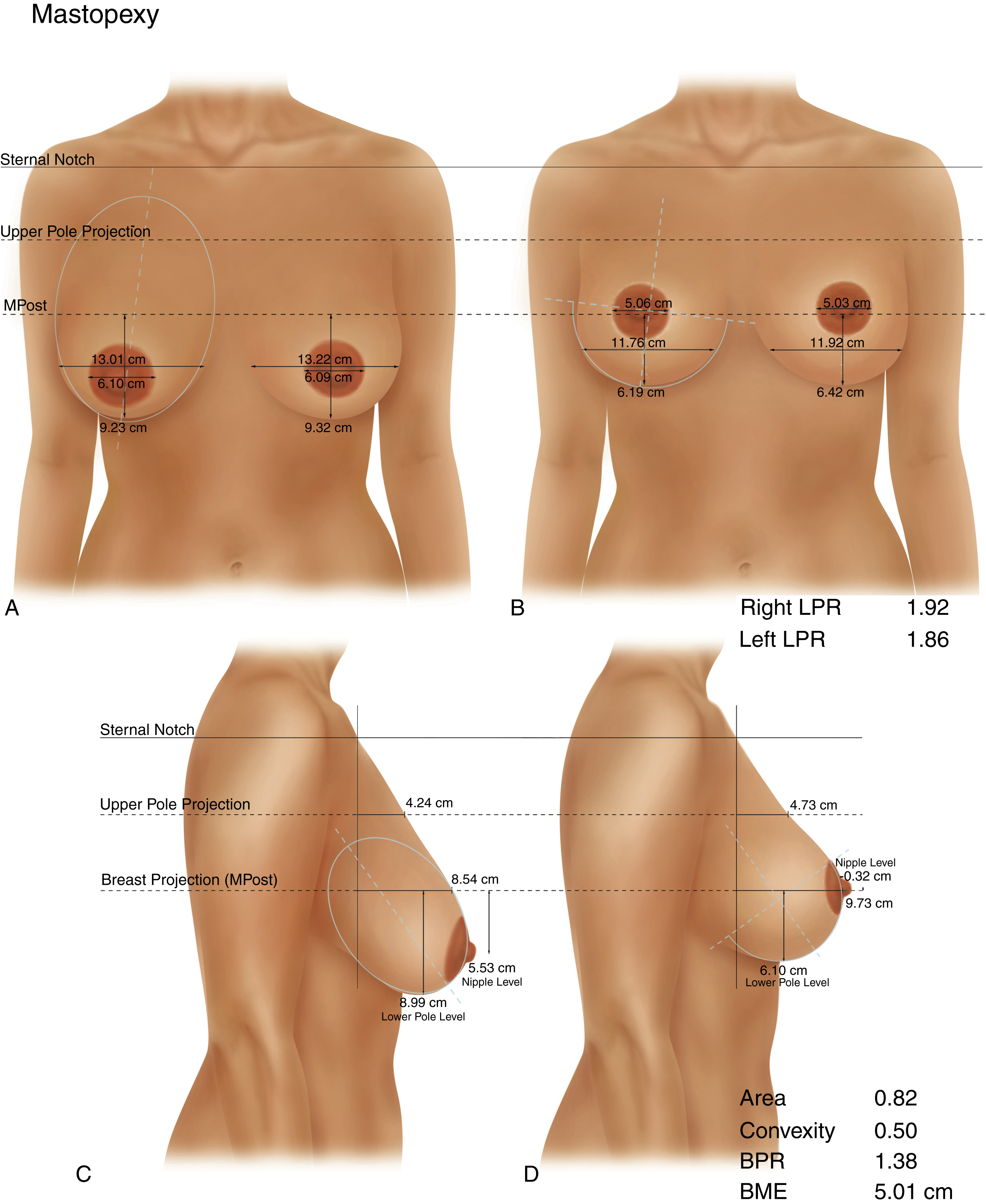
The mean increase in breast projection after vertical mastopexy is about 1.2 cm ( Fig. 14.1 ). Upper pole projection increases 0.5 cm, on average. These modest increases confirm the clinical impression that mastopexy and reduction cannot duplicate the effect of an implant in creating upper pole fullness.
Areola Diameter
The areolar diameter decreases approximately 1 cm after mastopexy. Patients do not favor large areolae. Despite using a 39-mm areola marking ring and an intraoperative positioning technique that theoretically reduces skin tension around the areola, areola diameters for the combined group of vertical mastopexy and reduction averaged approximately 5 cm after surgery, at the outside margin of the range deemed “okay” by patients. For this reason, an areola marking device with a diameter of 39 mm or less is recommended, allowing for a 1-cm stretch after surgery.
Lower Pole Level and Breast Mound Elevation
Vertical mastopexy elevates the lower pole level about 3 cm on average. Vertical mammaplasty effectively elevates the breast mound (level of maximum breast projection) about 4.7 cm. The nipple moves up 5.8 cm, on average. These measurements suggest that 80% of the upward nipple movement derives from breast mound elevation; 20% comes from nipple repositioning on the breast mound. This figure is calculated by dividing breast mound elevation by nipple elevation.
Surgical Technique
Relevant Surgical Anatomy
The intercostal perforating arteries from the internal mammary artery provide the dominant superficial circulation to the nipple and areola in 70% of women ( Fig. 14.2 ).
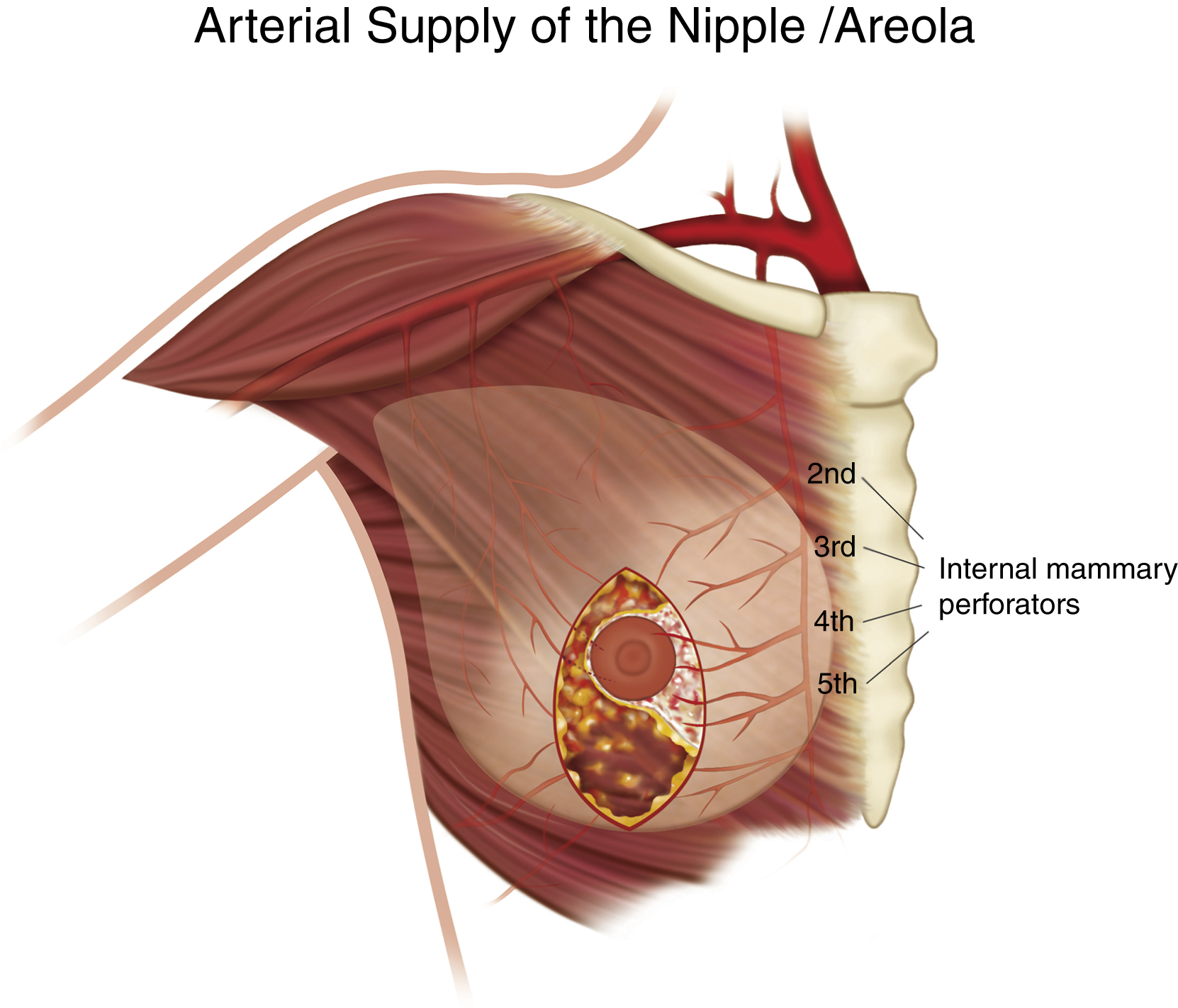
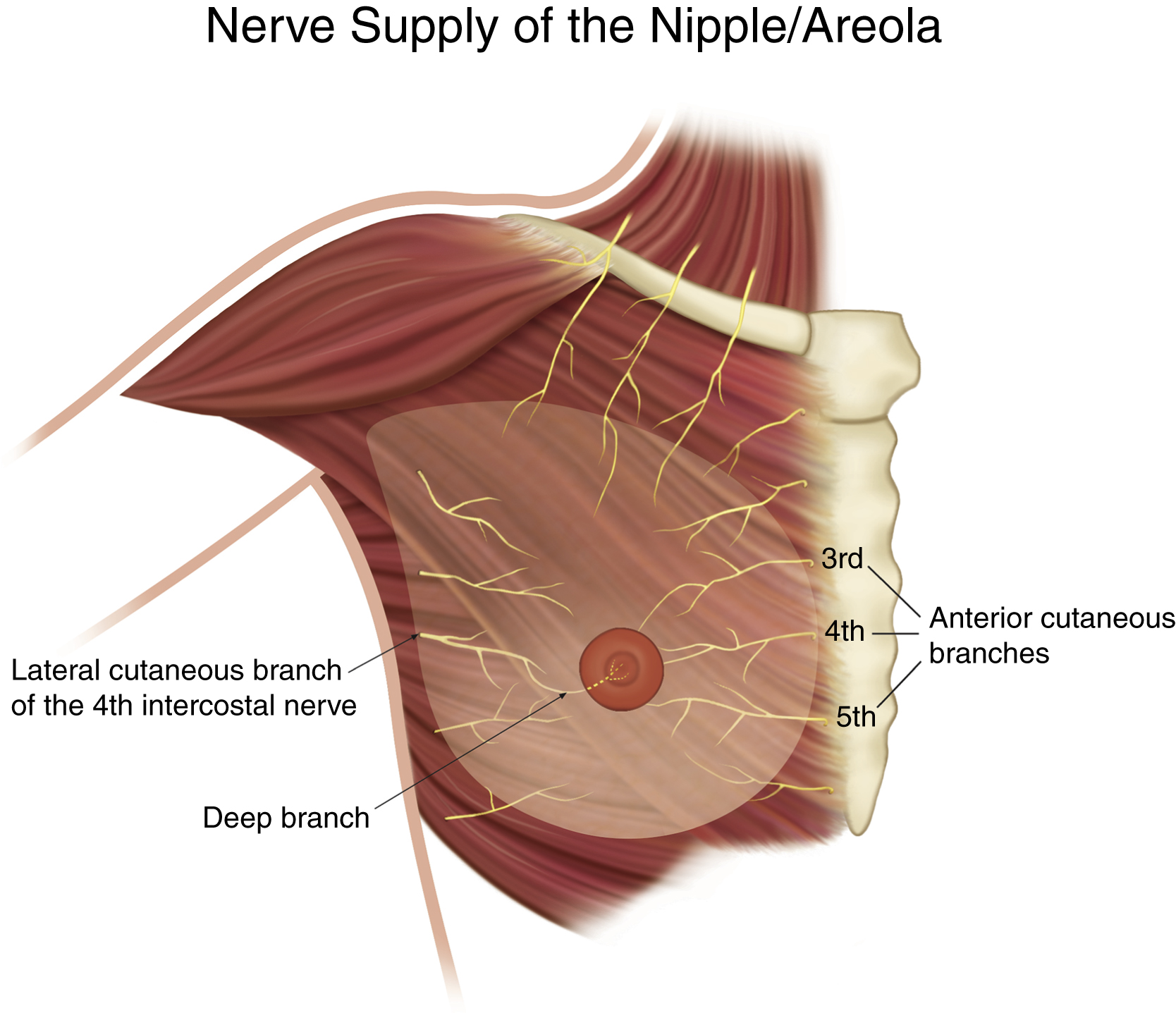
Superior and superomedial pedicles are popular. The advantage of a superomedial pedicle is inclusion of the second intercostal perforator. The advantage of the medial pedicle is ease of rotation and in-setting, which can occasionally be difficult when using a superior pedicle. Moreover, a medial pedicle preserves the medial anterior cutaneous innervation. By preserving a deep parenchymal attachment there is greater likelihood of maintaining innervation from the deep branch of the lateral branch of the fourth intercostal nerve ( Fig. 14.3 ). Superior pedicles are more likely to compromise sensation by sacrificing the deep innervation and by partially excluding superficial medial innervation. In choosing a medial pedicle, the author prioritizes nipple sensation, recognizing that perfusion is seldom a problem. Nipple sensation is important to women. A vertical mastopexy with a medial pedicle preserves nipple sensation in 90% of patients.
Preoperative Marking
Preoperative marking is performed with the patient standing. A measurement is made from the sternal notch, usually 21 cm. Next, the midline is marked at the xiphoid and an equidistant marking is made within each IMF (typically 10–12 cm). A vertical ellipse is marked. A mosque-dome or keyhole pattern is not used because the nipple position will be determined in surgery. The width of the ellipse is judged by folding in the lower pole tissue. A 10-cm width is common, but there is considerable variation depending on breast size, ptosis, and whether implants will be inserted simultaneously. The final determination is made in surgery. When they are used, breast implants are inserted first, before the mastopexy, so as to avoid overresection.
Anesthesia
Total intravenous anesthesia is administered. SAFE principles (Spontaneous breathing, Avoid gas, Face up, Extremities mobile) are observed. A laryngeal mask airway is used. No muscle relaxation is used to preserve the calf-muscle pump, an important consideration for preventing deep venous thromboses. A propofol infusion optimally maintains the mean arterial blood pressure.
Local anesthesia is injected in the form of 0.25% lidocaine, 0.125% bupivacaine, and 1:300,000 epinephrine. A volume of 60–100 cc per breast is injected. Both breasts are injected before the first incision is made to maximize the local anesthesia and epinephrine effect.
Surgical Technique
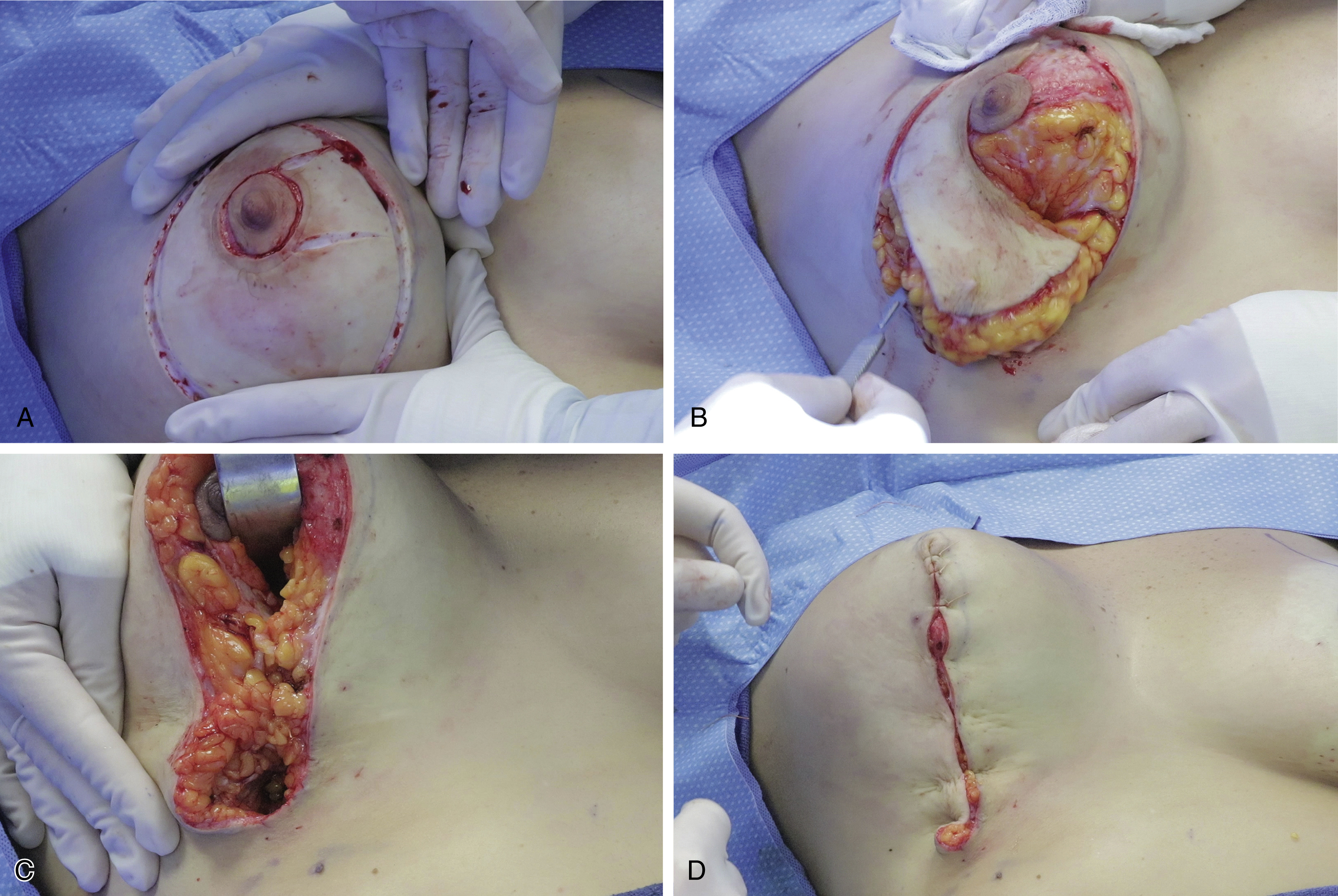
A video demonstrating a vertical mastopexy is provided (see  ). The video includes preoperative marking, details of the surgery and anesthesia, and follow-up 24 hours after surgery. The author’s mean operating time for a vertical mastopexy is 106 minutes. Intraoperative photographs of the same patient featured in the video are provided in Fig. 14.4 .
). The video includes preoperative marking, details of the surgery and anesthesia, and follow-up 24 hours after surgery. The author’s mean operating time for a vertical mastopexy is 106 minutes. Intraoperative photographs of the same patient featured in the video are provided in Fig. 14.4 .