Fig. 52.1
Functional zones of the retroperitoneum
Once an intra-abdominal venous injury is identified, you should immediately be planning out your potential operative strategies: to ligate the injured vessel, to shunt it, or attempt to repair it. All major abdominal veins are depicted in Fig. 52.2 and Table 52.1 and marked as amenable for ligation with relative impunity, ligate with consideration, and ligate in life-threatening scenarios only. All treatment decisions must be made in the context of the patient’s physiological condition at the time of laparotomy.
Fig. 52.2
Ligatable (white), potentially ligatable (gray), and preferably non-ligatable abdominal veins (black)
Table 52.1
Quick overview of management options while dealing with abdominal veins
Ligate with impunity | Recommendation |
|---|---|
Infrarenal IVC | Wrap and elevate lower extremities |
Common iliac vein | Wrap and elevate lower extremity |
External iliac vein | Wrap and elevate lower extremity |
Internal iliac vein | |
Inferior mesenteric vein | |
Splenic vein | |
Ligate with the following considerations | |
Right renal vein | Right nephrectomy |
Left renal vein, distal to gonadal vein | Left nephrectomy |
Hepatic veins | Follow-up liver ischemia |
Ligate only in lifesaving scenario | |
Suprarenal/perirenal IVC | Consider renal replacement therapy |
Superior mesenteric vein | Second look for gut ischemia |
Portal vein | Second look for gut ischemia |
52.1 IVC Injury
Approximately 1 out of every 50 patients with a gunshot wound to the abdomen will have an IVC injury. Prehospital mortality is close to 50 % and the survival of those who reach the hospital alive is reported to range between 20 and 40 %. Commonly, injury to the IVC will be associated with multiple visceral injuries. As a rule of thumb, the infrarenal IVC can be ligated, perirenal IVC ligation may result in nephrectomy/nephrectomies, and suprarenal IVC should be repaired, shunted, and/or packed if at all possible.
52.1.1 Exposure
Injury to the IVC presents at laparotomy with a hematoma or hemorrhage from Zone I, most commonly to the right of the midline. After evacuating the blood from the abdominal cavity and direct control of the hemorrhage with compression, consider aortic inflow control at the aortic hiatus. The next step is a right medial visceral rotation, which along with a Kocher maneuver will expose the entire infrahepatic IVC that may result in a major hemorrhage. For this very reason, before visceral rotation, ensure that you have multiple sponges on sticks, vessel loops, vascular clips, laparotomy pads, intravascular occlusion catheters, vascular instruments, and 4–0 vascular sutures on a large needle. Place a fixed retractor to maximize exposure, and warn your anesthesia colleagues that, in short order, a major hemorrhage may occur. Start the exposure by dividing the avascular colonic peritoneal attachments at the line of Toldt from the ileocecal region up to the hepatic flexure (Fig. 52.3). With an IVC injury, the blood will have tracked out laterally completing the majority of the dissection. The Kocher maneuver reflects the duodenum and the head of pancreas to the left facilitating the exposure of injuries of the perirenal/suprarenal IVC. Multiple options exist for controlling the IVC hemorrhage. The immediate goal is directed digital control of the injury or proximal and distal pressure on the IVC using sponges on a stick. With local control, vessel loops or vascular clamps can be used for more definitive control. With vascular clamps, one must be careful not to cause iatrogenic injuries when dealing with veins. If the injury is small, a side-biting Satinsky clamp may cover the entire length of the injury. Rapid control will minimize further blood loss and decrease the chance of air embolism. If tolerated, the Trendelenburg position prior to definitive repair may also obviate venous air embolism. If bleeding from the IVC continues after proximal and distal occlusion, the cause of bleeding is the lumbar veins. There are four to five pairs of lumbar veins entering the infrarenal IVC from the posterior aspect of the vessel. To access them, you need to rotate the IVC slightly and apply vascular clips, vessel loops, or ligatures on the lumbar veins. Dividing the lumbar veins after ligation improves the exposure of the posterior aspect of the IVC if necessary for repair. In repairing a wound of the perirenal IVC, you will also need to occlude the renal veins with vessel loops or vascular clamps.
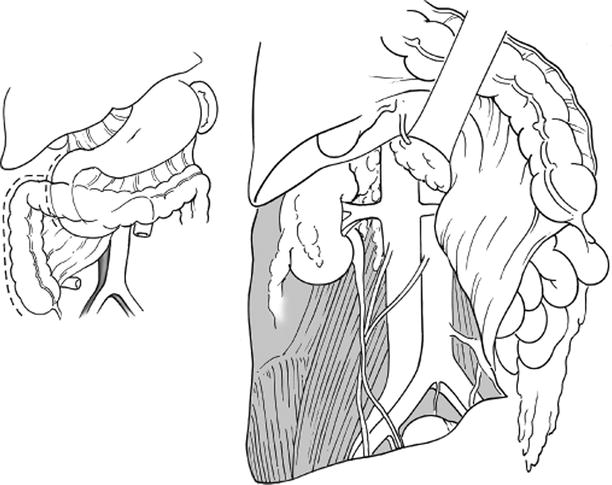
Fig. 52.3
Access to the infrahepatic inferior vena cava
52.1.2 Repair
There are numerous options for repairing the IVC (Fig. 52.4). Lateral repair is your first-line therapy. When using the side-biting Satinsky clamp, you may run a suture line along the clamp. If control was obtained with a laparotomy sponge, roll your compressive pads along the IVC, and, as soon as you identify the vessel edges, apply a Babcock clamp to close the visualized segment. Continue rolling your pad followed by the application of additional Babcock clamps until the vein wound is entirely clamped. The suture line can then run under the Babcock clamps removing each as the suture line progresses. In some instances, a missile will blow a larger hole into the IVC, and lateral repair will cause significant stenosis of the vessel (Fig. 52.5). If this stenosis approaches 50 %, consider repairing with a polytetrafluoroethylene (PTFE) patch. Always look for a through-and-through injury. Attempt to close this by rotating the vessel and ligating and dividing the lumbar veins if required. If this is not possible, another option is to extend the anterior wound and look for a posterior wound from within the vessel lumen. You should make every attempt to repair the suprarenal and perirenal IVC as ligation is associated with a high rate of renal failure. You may consider shunting the vessel if repair is not feasible as in a damage control setting. For infrarenal injuries, if the repair is highly complex or the patient is physiologically compromised, proceed with ligation.
Fig. 52.4
Inferior vena cava repair options
Fig. 52.5
Gunshot injury to the infrarenal inferior vena cava repaired with lateral venorrhaphy resulting in about 40 % stenosis (Courtesy of Dr. Talving)
52.1.3 Complications
The morbidity associated with IVC repair is due to venous stasis below the repair or ligation site. Elevation and wrapping of the lower extremities with elastic bandage alleviate the edema in the lower extremities. Long-term outcomes are very ill-defined. If there was visible stenosis at the time of repair, you may consider thrombosis prophylaxis when a patient is stabilized in the intensive care unit with low molecular weight heparin.
52.2 Portal Vein Injuries
Portal vein injuries are associated with an extremely high mortality ranging between 40 and 70 % among victims who arrive to the ED alive. Associated with the portal vein injury may be injury to the SMV, renal vessels, suprarenal IVC, pancreas, liver, biliary tree, or bowel.
52.2.1 Exposure
The portal vein starts at the confluence of the SMV and splenic vein behind the neck of the pancreas. After coursing behind the first portion of the duodenum, it enters the posterior aspect of the hepatoduodenal ligament. When dealing with a portal vein injury, you will notice either a hematoma or brisk dark hemorrhage in the supramesocolic central retroperitoneum either at the mesenteric root or in the hepatoduodenal ligament. Also, there may be massive bleeding from the wound in the pancreatic neck or head. Such venous bleeding can originate either from the suprarenal IVC or portal vein. Most commonly, portal vein injuries are combined with an injury to the suprarenal IVC. Again, you must be ready to obtain rapid local control of the vascular injury. The vast majority of those who reach the OR alive will exsanguinate during the exploration while unroofing the hematoma. Your primary aim is to arrest the bleeding by applying local compression and if required controlling the aortic inflow at the hiatus. Parallel to this, volume restoration with blood products requires constant communication with the anesthesia team. To approach the portal vein for suprapancreatic or retropancreatic injuries, the same exposure principles apply. Start with a right medial visceral rotation followed by a Kocher maneuver, which exposes the posterior and lateral aspects of the suprapancreatic portal vein (Fig. 52.6). While progressing with exposure, you are looking for three “B’s”: blood, bile, and/or bubbles consistent with bleeding, biliary tree, and/or duodenal injury, respectively. Divide the cystic duct, and attempt to obtain vascular control by identifying the injury and applying vascular clamps proximally and distally. Avoid iatrogenic injuries to the hepatic artery and common bile duct. Whereas many experienced trauma surgeons would discourage pancreatic division unless the injury has already been done so, if exposure does not allow the visualization of the injury, stapled pancreatic division may be required.