Fig. 33.1
The surgical anatomy of the superior mediastinum and neck indicating the proximity of the vessels and nerves around the aero-digestive tract
The neck contains many vital structures located in a small volume:
The important anterior structures of the neck lie deep to the platysma, and as a result, only injuries that have penetrated through this muscle are clinically significant.
As a result of the aero-digestive tract’s position in the midline and its close relationship to the major blood vessels in the neck injuries, crossing the midline usually causes a greater degree of damage.
The sternocleidomastoid muscle divides the posterior and anterior triangles of the neck. Within the anterior triangle lie the aero-digestive tract and the major blood vessels supplying the head and face, while the posterior triangle contains the nerves and blood vessels to the upper limbs.
The area of the neck posterior to the cervical vertebral body and the scalene muscles is composed mainly of muscle, bone and other nonvital structures. The spinal cord is encased in the cervical spine which usually can only be penetrated by gunshots.
The neck is divided into three zones using anatomic landmarks (Fig. 33.2). The management of injuries in these zones varies due to the vital structures that each zone contains and the manner in which access can be gained.
Fig. 33.2
(a) Zones of the neck, projected onto the cervical spine. (b) Zones of the neck and vascular structures
Zone I is the area between the clavicle/suprasternal notch and the cricoid cartilage, encompassing the thoracic outlet structures (Fig. 33.2a). The proximal common carotid arteries, internal jugular veins, vertebral arteries and veins and the subclavian arteries and veins and the trachea, oesophagus, thoracic duct and thymus are located here (Fig. 33.2b).
Zone II is the area between the cricoid cartilage and the angle of the mandible. It contains the internal and external carotid arteries; jugular veins; pharynx; larynx; oesophagus; cranial, sympathetic and recurrent laryngeal nerve; spinal cord; trachea and thyroid and parathyroid glands.
Zone III is the area that lies between the angle of the mandible and the base of the skull. It contains the distal extracranial internal carotid and vertebral arteries, the uppermost segments of the jugular veins and a variety of cranial nerves.
Tight fascial compartments of neck structures may limit external haemorrhage from vascular injuries, but it may increase the risk of airway compromise by an expanding haematoma.
33.1 Pathophysiology
Wounding instruments have specific characteristics that affect surgical findings. Two factors in the mechanism of injury or kinematics in penetrating neck trauma determine the extent of damage to the tissue:
Weapon characteristics:
Tissue injury results from either a direct impact by the penetrating projectile or tissue displacement from temporary cavitation caused by high-velocity projectiles.
Stab wounds typically have a 10 % higher rate of negative exploration than injuries from projectiles.
Secondary missiles in gunshots frequently add to the injury severity.
Location of injury and human tissues involved:
Wound sites and, if present, the wounding agent (retained bullet or stabbing implement) provide an indication of the likely injury complex.
Implied wound tract, particularly if it crosses the midline, is of particular value.
Penetrating injuries may cause partial or complete transection with thrombosis of the vessel or pseudoaneurysm. Pseudoaneurysm may have an acute or delayed onset with progressive enlargement causing compression of the surrounding structures. An arteriovenous fistula may develop if there is adjacent perforation of an artery and vein and is often accompanied by a pseudoaneurysm. Intimal injury can be caused by a high-velocity missile shock wave. The vessel is macroscopically intact with minimal bruising, but on opening the vessel, there is an intimal tear with or without a superimposed thrombosis.
The potential neurological consequences of vascular injuries are caused by hypoperfusion (caused by transected or thrombosed vessels) or embolisation from intimal injuries, pseudoaneurysm or AV fistulae.
33.2 Clinical Signs
Rapidly expanding cervical haematoma, absent carotid pulse, a bruit or thrill and external bleeding are hard signs indicative of vascular injury. Soft signs which may indicate a vascular injury and warrant further investigation include active or previous bleeding from wounds of the neck or the pharynx, a superficial temporal artery pulse deficit, ipsilateral Horner’s sign, IX–XII cranial nerve dysfunction and a widened mediastinum. Neurological deficit may be present, but obscured due to concomitant head injury, shock or the use of alcohol or drugs. Up to 50 % of patients with established blunt injury caused by cavitation to the carotid and vertebral arteries could initially be asymptomatic, but 43–58 % of these will eventually develop neurological signs. Physical exam is most reliable for arterial injuries, but less sensitive to venous and aero-digestive tract injuries. The presence of distal pulses does not rule out an arterial injury. Be aware of concomitant injury to nearby structures. Signs of laryngeal injury include respiratory distress, stridor, subcutaneous air, haemoptysis, odynophagia and anterior neck pain. Dysphagia, bloody saliva, subcutaneous air and haematemesis are all features suggestive of oesophageal injury. Neurological fallout will vary depending on the affected segment.
33.3 Management
33.3.1 The Stable Patient: Diagnostics – CT Scan or Equivalent
Patients with active bleeding and a compromised airway require immediate exploration. Occasionally, such bleeding can be controlled with insertion of a Foley catheter, thereby converting this extremely dangerous setting to a semi-elective one.
Haemodynamically stable patients with a patent airway who have the following signs should undergo further appropriate investigations:
In gunshot injuries:
Proximity to vessels
Evidence of crossing the midline
Bleeding that has been controlled by a Foley catheter or similar manoeuvre
In stab wounds:
Wound penetrating platysma and with bleeding that has been controlled by a Foley catheter or similar manoeuvre
The diagnostic modalities used are:
Duplex Doppler examination is useful for investigating zone II vascular injuries. Duplex scanning, however, has its limitations in zones I and III due to anatomical constraints. Duplex Doppler is not as readily available at all times and requires an experienced operator.
Multislice contrast CT and CTA has replaced arteriography in recent years, as it not only demonstrates vascular anatomy well but also gives substantial additional information about other structures in particular those of the aero-digestive tract. A review by Woo and colleagues reports that the use of CTA is associated with less operative exploration, less negative explorations and reduced use of invasive studies, such as conventional angiography. Physical examination findings supplemented by CTA should have a prominent role in the selective management of penetrating neck injuries. CTA has replaced angiography as the initial study of choice in the vascular evaluation of a neck injury (Fig. 33.3).
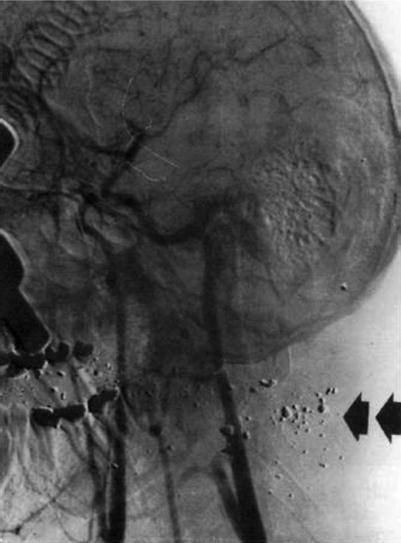
Fig. 33.3
CTA has replaced angiography as the initial study of choice in the vascular evaluation of a neck injury (here in patient with fragmented gunshot neck) Arrows indicate bullet fragments and injury tract with external carotid injury
A CT scan of the brain should be obtained to investigate patients with associated head trauma, bone injuries of the spine and skull and those with neurological deficit. A CT scan of the brain is a good predictor of outcome: Patients who have an infarct on initial CT on admission have a high mortality with poor chance of neurological recovery compared to those patients who have a normal CT on admission.
Arch angiography remains a good alternative if CTA is not available for the diagnosis of cervicomediastinal (zone I) and zone III vascular injuries. It gives information regarding suspected injuries to other vessels and evaluation for possible endovascular treatment. Certain centres that have in-house angiographers may perform angiography for injuries in zone I and zone III despite hypotension or haemorrhage. Angiography remains the criterion standard for defining arterial anatomy and injury complexes, with an accuracy close to 100 % (arteriography demonstrates a low yield in asymptomatic patients). Arteriography is usually performed using a digital subtraction angiography (DSA) technique that reduces the amount of contrast required and yields a superior computer-manipulated image for evaluation.
MR angiography may be valuable in carotid artery and vertebral artery dissection but only in the stable patient, as monitoring of the vital signs is difficult during the investigation and MRA is a time-consuming investigation.
Cervical anteroposterior and lateral radiography with bullet markers is used to evaluate for vertebral bony injury; retained foreign bodies; and foreign body deformity, location, size and number. These radiographs can also give additional valuable information like retropharyngeal or mediastinal air which are indicative of aero-digestive tract injuries.
33.3.2 The Unstable patient: Operative Approach
33.3.2.1 Management in the Emergency Department
Advanced Trauma Life Support (ATLS) guidelines should be followed for severe cervical vascular injuries. Thus, airways with cervical spine control and respiration have first priority, followed by control of bleeding. Control of bleeding is best achieved by manual compression or application of a Foley catheter (see later) applied directly to the bleeding site. Blind application of haemostatic clamps should not be attempted because of the risk of injuries to blood vessels as well as to other structures. Do not remove impaled objects until the patient is in a controlled environment and you are ready to control the bleeding.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


