Artery
Primary repair
Graft or vein
Ligate?
Recommendations
Aorta
Prolene 3-0 or 4-0
Dacron 14–20 mm
No
Prefer left medial visceral rotation exposure
Splenic
N/A
N/A
Yes
Splenectomy
Common hepatic
Prolene 5-0 or 6-0
Saphenous vein graft
Yes
Need intact portal vein
Cholecystectomy
Celiac axis
Prolene 5-0 or 6-0
N/A
Yes
Ligate
SMA
Prolene 5-0 or 6-0
Vein preferred
No
Ligate in lifesaving scenario only
Shunt whenever possible for damage control
IMA
Prolene 6-0
N/A
Yes
Ligate
Common iliac
Prolene 4-0 or 5-0
PTFE ≥6 mm
No
Shunt or immediate bypass
Watch for need of leg fasciotomy
External iliac
Prolene 4-0 or 5-0
Vein or PTFE ≥6 mm
No
Shunt or immediate bypass
Internal iliac
Prolene 4-0 or 5-0
N/A
Yes
Ligate
Renal
Prolene 5-0 or 6-0
Vein or PTFE
No
Nephrectomy if ligation required
Ensure contralateral kidney function prior to ligation
Mesentery (unnamed)
No
N/A
Yes
Ligate with impunity
Explore all hematomas for arteries in spasm that need ligation
The shunt is an important tool to keep in your back pocket. It is a rapid, inexpensive, technically simple tool that allows you to follow the underlying principle in vascular trauma which is to restore blood flow and reperfuse ischemic tissue or organs. If the patient begins that downward spiral of the lethal triad and the vessel that is bleeding can be ligated, ligate. If not, get a shunt into the vessel, restore flow, and proceed to the ICU. A shunt can be anything from a feeding tube for smaller vessels to a chest tube for a large vessel such as the aorta. Typically, we use commercially available and purpose-designed vascular shunts at our institution; however, any hollow tube is acceptable, ensuring it is slightly smaller than the vessel lumen so as to not damage the endothelium. A silk tie is secured to the center of the shunt to mark the middle and prevent shunt migration. After placing the middle silk tie, slip the proximal and distal ends of the shunt into the respective ends of the injured vessel. Keep in mind that the segment of the vessel that is tied down to hold in the shunt will be damaged and will have to be removed during definitive repair. Therefore, do not trim or debride the injured vessel prior to shunt insertion to maximally preserve native vessel length. In addition, secure the shunt as close as possible to the end of the injured vessel so as to preserve length. In general, the flow drives shunt patency and anticoagulation is not used, as patients requiring damage control shunting often have diffuse nonsurgical bleeding which may be exacerbated by this. You have now restored flow and can bring the patient safely to the ICU for further resuscitation.
After the patient is adequately resuscitated, acidosis corrected, and hypothermia eradicated, you are now ready to return for definitive repair of this vessel which can be a simple primary repair or more involved with an interposition graft comprising the saphenous vein or a synthetic graft.
53.3 Retroperitoneal Hematomas: Plan of Action
When discussing abdominal bleeding and the trauma exploratory laparotomy, it is common to refer to the areas of hematoma that will help you plan your exploration. The retroperitoneum is divided into four areas: zones I–III and zone IV, the retrohepatic area (Fig. 53.1). The retrohepatic area is composed of the hepatic veins and retrohepatic IVC and thus will not be discussed in this chapter.
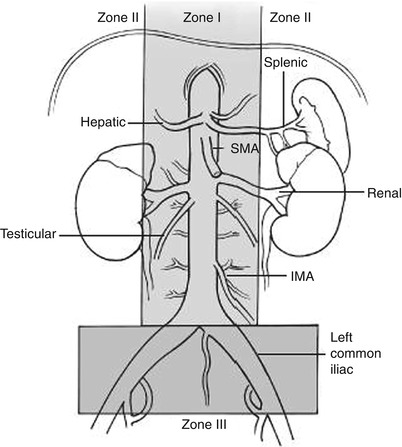
Fig. 53.1
Anatomical vascular regions
53.3.1 Zone I
Zone I refers to a central retroperitoneal hematoma. A hematoma in the supramesocolic location suggests that the suprarenal aorta, celiac, or superior mesenteric artery (SMA) may have been injured, while an inframesocolic location would suggest injury to the distal SMA or infrarenal aorta.
53.3.1.1 Aorta
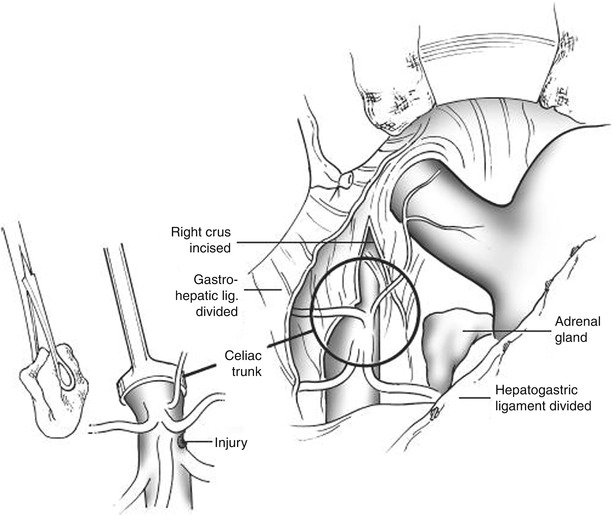
The suprarenal aorta can be accessed by a left medial visceral rotation also known as the Mattox maneuver. This can expose the entire length of the aorta and its branches to include the celiac axis, superior mesenteric artery, and inferior mesenteric artery. After making your midline incision from the xiphoid to the pubis, take down the falciform ligament posteriorly making sure to stop short of the hepatic veins. The Balfour retractor is a simple instrument for retracting the abdominal wall. For larger patients or for areas such as the iliac vessels, a large fixed retractor may be required. Reflect the omentum and transverse colon superiorly, eviscerate the small bowel to the right, and find the sigmoid colon. Lift the sigmoid colon up into the field, and start your dissection on the white line of Toldt (aka the peritoneal reflection). Once the peritoneum is taken down, your hand can easily dissect through the loose areolar tissue in the retroperitoneal space, especially if blood has dissected through the soft tissue planes. Continue this dissection superiorly keeping on top of the psoas muscle to include the descending colon, splenic flexure, stomach, spleen, and pancreatic tail. This will allow you to bluntly lift up these structures and mobilize them into the midline. At this point, the aorta and its branches can be visualized.
If bleeding is not adequately controlled with direct pressure and cross clamping of the aorta is your next move, the supraceliac aorta should be accessed. Keep in mind that inflow control will cause ischemia to all structures distal; thus, the time the cross clamp remains on the aorta needs to be kept as short as possible. The longer the clamp remains in place, the more difficult removal becomes and the more profound the reperfusion effect. For intra-abdominal supraceliac control, direct compression manually is best, especially if there is sufficient blood pressure to allow for easy palpation of the aorta as it exits the chest. If dissection is required or if you are going to attempt clamp placement, cutting the left crus of the diaphragm (at 2 o’clock to avoid bleeding) will facilitate exposure. Using your fingers, bluntly dissect away the dense neural and fibrous tissue over the aorta and create a space on either side. You may attempt to place a large vascular clamp across the aorta. If successful, secure the clamp so that it cannot fall off or be knocked off inadvertently. Practically however, it is usually very difficult to keep the clamp in place because it slips off easily. What we recommend for better control of the aorta is direct compression of the aorta against the vertebral bodies. This can be achieved by a compression device, a sponge stick, or your assistant’s hand (Fig. 53.2). In rare instances with high supramesocolic injuries, the safest way to achieve proximal aortic control is through a left thoracotomy.