83
Macrodactyly
Ann E. Van Heest and James House
History and Clinical Presentation
A 5-month-old boy presented with an enlarged left middle finger. He was born at 38 weeks’ gestation by normal vaginal delivery, weighing 7 lb, 9 oz. The pregnancy was complicated only by preterm labor at 32 weeks that was successfully managed with bed rest and medication. The diagnosis was made at the time of delivery. The child had no other medical problems. All developmental milestones were achieved normally. Family history was negative.
Physical Examination
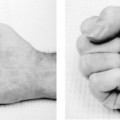
The child has an enlargement of the left middle digit, involving primarily the phalanges (Fig. 83–1). He can actively flex and extend the digit, but is limited at the interphalangeal joints by the soft tissue bulk of the digit. A soft tissue enlargement could be palpated proximal and distal to the transverse carpal ligament in the palm and in the distal forearm, consistent with enlargement of the median nerve. In comparison to the mother’s hand, the child’s distal phalanx and nail appeared to be almost the same size. In comparison to the child’s right hand, the other digits of the left hand do not appear to be involved. The child had no skin lesions. The physical examination was otherwise normal.
PEARLS
- Early intervention with epiphysiodesis has been effective in preventing longitudinal overgrowth.
- Epiphysiodeses should be performed when that segment of the child’s digit is approximately the same size as the same gender parent.
- For circumferential bulk reduction, surgery should be performed in two stages with debulking on one side in the first stage, and debulking on the other side of the digit as a second stage in 3 to 6 months.
- Individualize the treatment plan based on the degree and extent of the deformity.
- If the size is significant and the function poor, recommend amputation early, prior to multiple operative interventions.
PITFALLS
- Nerve resection has not been helpful in preventing overgrowth.
- A complete physical examination and screening radiograph are necessary to screen for syndromic involvement.
- Parents need to be counseled that surgical intervention will debulk the digit, but will not make the digit look normal. Residual scars, stiffness, and the need for multiple operations are common.

Figure 83–1 Macrodactyly of the middle digit with greater involvement distally than proximally is present in this child. The enlargement involves all elements of the soft tissue as well as the skeleton.
Diagnostic Studies
The anteroposterior (AP) radiograph showed soft tissue and bone enlargement of the middle digit of the left hand, involving primarily the phalanges (Fig. 83–2). The enlargement is greatest distally, with progressively less involvement proximally.
Differential Diagnosis
Macrodactyly
Nerve tumor
Vascular malformation
Proteus syndrome

Figure 83–2 Anteroposterior (AP) radiograph shows the middle digit with enlargement of the phalanges and minimal involvement of the metacarpal. Associated soft tissue enlargement is noted.
| Macrodactyly | Idiopathic, isolated event; lipofibromatous hamartoma of the associated peripheral nerve |
| Proteus syndrome | Macrodactyly hemihypertrophy, pigmented nevi, subcutaneous tumors (lipoma, hamartomas), skull anomalies (osseous protuberances, craniosynostosis, macrocephaly); may include spinal deformity, angular limb deformities, hip dysplasia, joint contractures |
| Neurofibromatosis | Autosomal dominant, macrodactyly, multiple neurofibromas, cafe-au-lait spots |
| Klippel-Trénaunay-Weber syndrome | Hemihypertrophy, port-wine cutaneous hemangiomas, arteriovenous fistulas, inadequate deep venous system with varicose veins |
| Maffucci or Ollier’s disease | Overgrowth associated with enchondromas |
Digital overgrowth can occur as an isolated event or as part of a syndrome (Table 83–1
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


