Lymphedema Microsurgery for Breast Cancer-Related Upper Limb Lymphedema
Ming-Huei Cheng
Jung-Ju Huang
DEFINITION
Lymphedema can be inherited or a complication after lymph node dissection. Breast cancer-related lymphedema (BCRL) is a potential complication after axillary lymph node dissection, particularly in patients who have or will receive adjuvant radiation.
With the subcutaneous accumulation of lymphatic fluids, the typical early sign of lymphedema is swelling of the affected limb. Occasionally, patients may present with pain as the first symptom of lymphedema.
Definitive diagnosis can be confirmed by lymphoscintigraphy.
ANATOMY
There are approximately 600 to 700 lymph nodes located in a human body, and the axilla is one of the most concentrated areas.
PATHOGENESIS
The lymphatic system maintains fluid homeostasis, absorbs dietary fat, and facilitates the host immune response. Once disturbed, fluid homeostasis is blocked and subsequent disease is initiated.
Unbalanced fluid homeostasis can cause protein-rich fluid to leak into the interstitial tissue, resulting in swelling, local tissue inflammation, adipose deposition, and fibrosis.
A compromised local immune defense makes a patient more susceptible to infection, and repeated cellulitis is one of the common features of lymphedema.
Although breast surgeons have reduced the frequency of axillary dissection through the use of sentinel lymph node biopsy (SLNB), upper extremity lymphedema can still occur after SLNB or ALND.
NATURAL HISTORY
BCRL is the major factor that compromises a breast cancer patient’s quality of life after treatment.1
The presentation time and symptoms of lymphedema are highly variable among patients.
Risk factors that contribute to the severity of lymphedema other than radiotherapy include infection and obesity.
As it differs from most traditional treatments that involve excision or other destructive procedures, microsurgical treatment for lymphedema aims to drain the accumulated fluid from the affected extremity.
Lymphaticovenous anastomosis (LVA) is the first microsurgery procedure to treat lymphedema.
However, this approach has not been popular until recent years, as more accurate diagnostic tools to identify lymphatic vessels have become available, such as indocyanine green (ICG) lymphography.3
Another microsurgical treatment is vascularized lymph node transfer, which was first developed in an animal study in the 1990s.
The idea of transferring healthy, unaffected lymph nodes from other donor sites to the affected extremities provides another approach for microsurgical lymphatic fluid drainage once the lymphatic vessels are destroyed and LVA is not possible.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients with BCRL may experience discomfort, swelling, and recurrent cellulitis of the affected extremity.
The first sign of lymphedema is often swelling.
Occasionally, they present with intractable pain for an unknown reason or with repeated cellulitis.
The resultant problems may become both a physical and psychosocial problem.
Physical examinations of a lymphedema-affected extremity often reveal nonpitting swelling and thickening of the skin (which can be peau d’orange skin or even woody in more advanced stage).
It is not uncommon to find skin erosion or ulceration or signs of infection on the skin.
Occasionally, brachial plexus dysfunction can occur.
With long-term involvement, the skin of the affected extremity can present elephantiasis nostra verrucosa, which appears hyperkeratotic with cobblestonelike skin and some papillomatous plaques.
Clear or light yellow fluid can ooze from the skin.
The tissue may become malodorous in the setting of poor hygiene.
IMAGING
Accurate diagnosis and grading of lymphedema help to identify suitable treatments.
Measurement of the limb circumference and calculation of the difference between the normal and diseased extremity often appears to be the first, easy diagnostic tool.
The level for measurement by the authors includes 10 cm above and below the elbow. The circumference difference can then be calculated accordingly (FIG 1).
Lymphoscintigraphy remains the standard diagnosis for lymphedema.
With the injection of a tracer molecule with technetium-99m into the dermis of a distal hand, the traveling of Tc-99 can be traced. Information regarding the clearance of the injection tracer, obstruction status (such as total or partial obstruction), and possible obstruction level/presentation of dermal backflow can be provided.
With a similar injection technique, ICG (indocyanine) dye is intradermally injected into the distal hand (often the 2nd and 4th web spaces).
With an infrared light source and diagnostic devices, such as PDE (Hamamatsu Photonics, Hamamatsu City, Japan), SPY (Novadaq Mississauga, Canada), and infrared detector-incorporated microscopy, the traveling course of the ICG dye (mainly inside the lymphatic vessels) can be identified. ICG lymphography provides a dynamic and panoramic view of the lymphatic drainage with time. It is a powerful tool for both lymphedema diagnosis and intraoperative planning for lymphatic surgery.
The main drawback is that the detection of the ICG is limited to approximately 1 cm underneath the skin.
DIFFERENTIAL DIAGNOSIS
Diseases other than lymphedema can present with swelling of extremities, such as mechanical obstruction and venous thromboembolism.
Ultrasonography to assess the status of venous drainage is recommended.
NONOPERATIVE MANAGEMENT
Nonoperative management strategies include manual massage, complex decongestive physiotherapy (CDP), and compression garments.
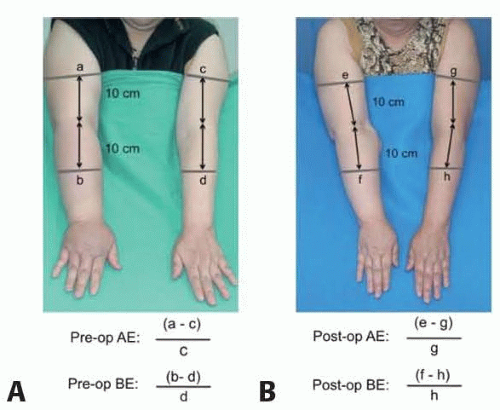 FIG 1 • Measurement of volume differentiation of circumference before (A) and after (B) lymphedema surgery. To do this, the circumferences of the upper arm and forearm are first measured at the level of 10 cm above and below the elbow. |
SURGICAL MANAGEMENT
Microsurgical treatment for BCRL includes LVA, vascularized lymph node transfer (VLNT), and the combination of microsurgical breast reconstruction and lymph node transfer using an abdominal flap with superficial groin lymph node transfer.
A “Barcelona cocktail” is a combination of microsurgical breast reconstruction with superficial groin lymph node transfer to the axilla and LVA in the forearm, which aims to complete surgical treatment at one stage.
Early interventions provide better recovery because the pathological progress of adipose deposition and fibrosis can be better prevented. This is especially true when LVA is considered.
Microsurgical treatments may not achieve the same degree of volume reduction as liposuction; instead, they gradually stop the disease progression by effectively draining lymphatic fluid into the venous system.
Patients with fibrosis may still benefit from surgery with adjuvant procedures, such as liposuction and/or partial soft tissue resection.
The selection of treatment is based on the severity of lymphatic obstruction and clinical symptoms (FIG 2).
Lymphaticovenous Anastomosis
Technological advancements in diagnosis and mapping have allowed LVA to become a popular procedure for lymphedema treatment in early-grade cases with promising results.
Different surgeons have different preferences for performing LVA, including the method (end-to-end, end-to-side, and side-to-end), locations, and numbers of LVAs that have to be done.
Supramicrosurgery, including anastomosis of vessels as small as 0.8 mm or less to small subdermal veins, has been recommended.4 To prevent postoperative venous reflux, a suitable recipient vein should present with minimal backflow after it is cut. Strong backflow from the subdermal veins may result in venous blood backflowing into the lymphatics. This results in a limited chance for lymphedema recovery, ecchymosis, and discomfort.
Vascularized Lymph Node Transfer
There are two different theories supporting its mechanism for lymphatic drainage.
One is based on lymphangiogenesis and spontaneous lymphatic connection.7
The other is based on the inherent lymphaticovenous connection inside the flap.8
Cheng and colleagues demonstrated in animal studies and intraoperative images evidence to support their theory of this mechanism.9 By injection of ICG dye into the subcutaneous tissue of lymph node containing flaps, ICG is eventually drained via the flap donor vein.
Conversely, drainage is absent when the dye is injected into non-lymph node-containing flap.9 They have demonstrated that the inherent lymphaticovenous connection is the main mechanism for lymphatic drainage. Combined with “catchment effect” and “gravity” effect, VLNT placed in the distal recipient site would offer the most benefit for lymphatic drainage.
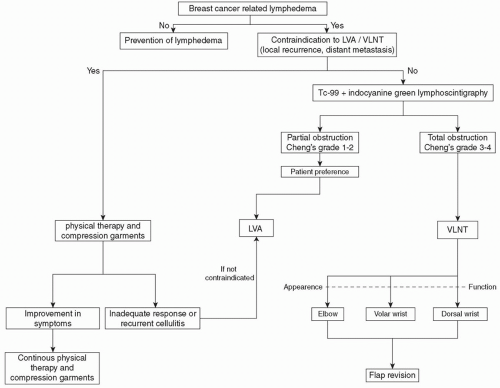 FIG 2 • Algorithm for surgical approaches of breast cancer-related lymphedema (BCRL). |
Preoperative Planning
Cheng and colleagues developed a disease grading system that includes both clinical symptoms and diagnostic results from lymphoscintigraphy6 (Table 1). Based on the staging system, patients are graded from 0 to IV according to the lymphedema severity.
By combing preoperative symptoms and diagnostic findings, mainly lymphoscintigraphy and ICG lymphography, an algorithm has been developed to more accurately assign the patients to appropriate treatment (see FIG 2).
If the lymphatic obstruction is partial and functional lymphatic vessels can still be identified in ICG lymphography, LVA can be considered a good surgical option.
However, if the lymphatic obstruction is complete and functional lymphatics are not identifiable, VLNT is the best surgical option.
Patients who have stage III or IV lymphedema usually require additional procedures other than microsurgical treatment to optimize the results.
Patients showing a linear pattern of lymphatic vessels with ICG lymphography can be selected for LVA with predictably good outcomes.
The preoperative use of duplex ultrasonography aids in the selection of the optimal flap for VLNT.8 Additionally, duplex ultrasonography can be useful in determining recipient vessels for VLNT.8
More detailed preoperative examinations, such as computer tomography (CT) scan or magnetic resonance imaging (MRI), can be helpful to further differentiate the disease pathology and identify the donor and recipient vessel quality.
Positioning
Patients are in the supine position for both LVA and VLNT.
Hyperextension of the neck is required if submental lymph node flaps or transverse cervical lymph nodes are selected as donor sites.
Approach
For LVA, surgical approach includes one to several 3-cm incisions, depending on preoperative ICG lymphography.
Surgical approach for VLNT includes flap harvest and recipient site preparation. There are many donor flaps for VLNT depending on preoperative evaluation and the surgeon’s preference. Advance selection of appropriate recipient site is equally important (proximal vs distal on the extremity).
Some surgeons place the VLNT into the axilla where a previous axillary scar exists. The scar will need to be fully
released during VLNT. However, we prefer to place the lymph node flap in a more distal recipient site.
A distally transferred lymph node flap may function better than proximally transferred lymph node flaps. One possible explanation could be that with disease progression, gravity draws the fluid to a more dependent site.
In contrast to the need for a compression garment after surgery in patients receiving lymph node transfer to the axilla, the authors do not recommend a compression garment for patients with a distally transferred lymph node flap. We believe that omitting a compression garment is also an important part of enhancing the quality of life after lymphedema treatment.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree