Previously, abnormalities of the upper eyelid such as crease asymmetry and hollow sulcus, were treated surgically, if at all. Injecting hyaluronic acid (HA) filler to the upper lid can correct a hollow sulcus, improve the lid crease, and reduce tarsal platform show. In the lower lid, precise injection of HA filler can be used to correct post-blepharoplasty lid retraction with long-lasting results.
Key points
- •
HA filler can correct superior sulcus hollowing and decrease tarsal platform show.
- •
HA filler can be useful in correcting post-blepharoplasty lower lid retraction instead of surgery.
- •
Tarsal platform show is an important aesthetic component when evaluating upper eyelids.
Introduction
For a long time, it was common practice to perform subtractive blepharoplasty for patients seeking to undergo upper lid rejuvenation. Standard subtractive upper blepharoplasty procedures may lead to initial pleasing results for the patient and surgeon. However, over time, these patients can appear sunken or hollow, skeletonized. In recent years, we have come to appreciate the role of volume preservation or contouring in lower eyelid and cheek surgery. This concept has been less appreciated in upper lid evaluation, but is no less important for achieving esthetically-pleasing results. If one looks closely at pictures of the aging face, it is important to note a hollow superior sulcus which occurs with aging. When patients present, and use their finger to digitally elevate the upper eyelid skin, the author always advises them to look together with me at photos when they were younger. Invariably, they realize that they indeed had a full superior sulcus [ ].
Another important and related concept in the upper lid is tarsal platform show (TPS)—the distance between the eyelid crease and the lid margin or lash line. Studies have shown that TPS is one if not the most important factor when evaluating eyelid esthetics [ , ]. These studies have further shown that less TPS is esthetically preferable. TPS is determined by the eyelid fold and the eyelid height. TPS is increased in patients with ptosis and decreases as the eyelid is elevated in ptosis repair. In patients without ptosis, TPS is affected and determined by the lid fold.
While there is a role for excising or tightening tissue in the upper lid, the upper blepharoplasty surgeon should always be aware of the importance of the lid fold and the degree of TPS. Along this line of thinking, care should also be taken when addressing the fat pads in the upper lid. The nasal fat pad generally increases in size with age while there is hollowing of the central pads. In most cases, when performing upper blepharoplasty, only the nasal fat pad needs to be sculpted or removed. Central fat is rarely excised. In cases where there is prominent ptosis or micro-ptosis, elevating the lid (ptosis repair) should be performed as well in order to create volume, enhance the lid fold and reduce TPS.
We have discussed concepts of upper blepharoplasty here in order to be able to correctly treat the patient that presents with post-upper blepharoplasty hollowing, naturally occurring hollow sulci, and/or the patient with ptosis who asks for a blepharoplasty. Over-aggressive upper blepharoplasty can result in a hollowed-out appearance in the upper lid as well as asymmetric lid creases. The patient may also suffer from pre-existing ptosis which was not recognized pre-operation, or worsening ptosis post-operation. Patients may be subconsciously aware of increased TPS, without being to articulate it. But the resulting increased TPS only adds to the “tired” look and patient dissatisfaction.
For the patient with purely asymmetric lid creases and stable lid folds following upper blepharoplasty, it is important to discuss with the patient which crease height they prefer. In general, it is easier to raise a low crease compared to lowering a high crease. To raise a crease, the new, more superior crease is marked. After incision, dissection is carried out inferiorly in the pretarsal plane toward to lid margin, posterior to the current lower crease. Crease-forming sutures are then placed at the level of the new incision, in order to “stretch” the tissue out superior to the old crease with closureosure in a standard fashion. To lower a high crease, there first must be residual tissue to excise in the lid. The position of the lower, desired crease is marked, along with an ellipse which encompasses the higher crease. The high crease will be removed within the ellipse. Closure with crease-forming sutures is carried out.
If there is ptosis resulting in increased TPS, as well as asymmetric creases, then ptosis repair can be carried out. After advancement of the lid, crease forming sutures can be placed, controlling the position of the crease. If a patient with ptosis and increased TPS responds well to instillation of phenylephrine drops, the margin-reflex-distance (MRD) will increase and TPS decrease. This can also assist in evening out the creases, which may appear asymmetric from the ptosis. In patients with elevated lids after phenylephrine drops, this can produce a simulation for both the surgeon and patient. In these cases, the Muller muscle conjunctivital resection (MMCR) is a very useful procedure and can avoid another upper lid incision ( Fig. 1 .) The MMCR can be performed without sutures, which is a rapid procedure with quick recovery time with excellent results [ ].
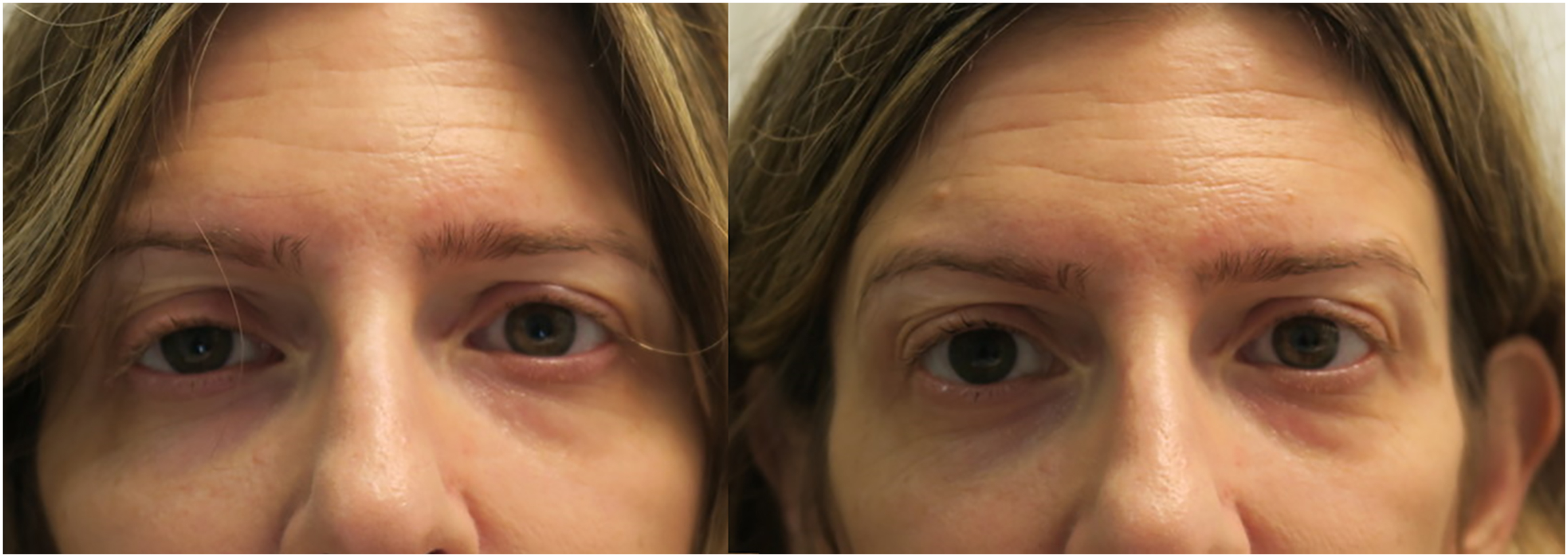
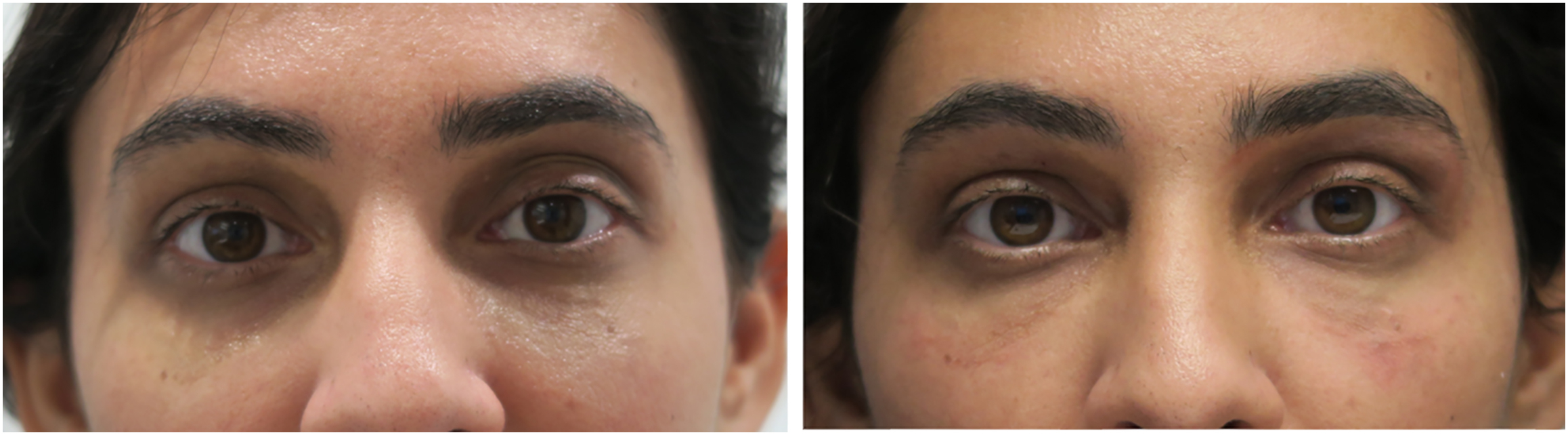
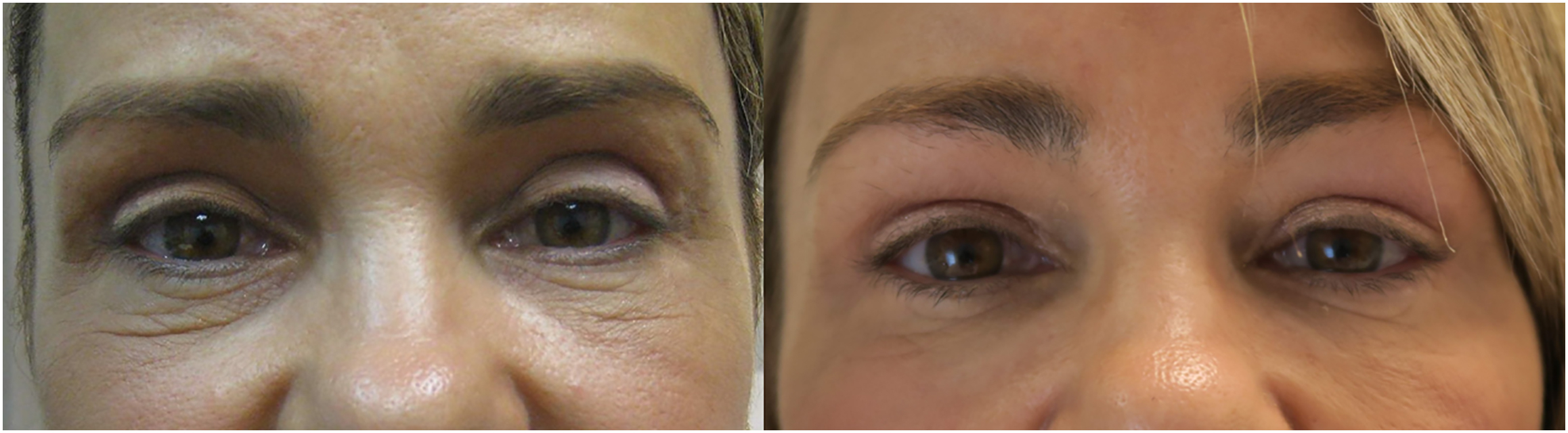
In recent years we have seen the advent of hyaluronic acid (HA) filler injections, which have been an immensely useful tool in rejuvenating upper lids. By carefully filling the hollow superior sulcus, the natural fullness of the lid can be restored, TPS can be decreased, and asymmetric creases can be corrected. This can all be carried out in a relatively short office visit, thus avoiding further surgery. Using HA filler is a relative quick in-office procedure with a short recovery time and high patient satisfaction. Fillers for the upper lid should not be too dilute as the filler may diffuse through the thin eyelid skin and cause edema. More concentrated fillers can lead to lumps and bumps. Thus, moderately concentrated fillers, similar to those used in the lower lid are appropriate for the injections in the upper lid (Restylane Refyne, Galderma, Lausanne, Switzerland; Teosyal Redensity II, Teoxane, Geneva, Switzerland; Belotero Intense, Merz Pharma KGaA, Frankfurt/Main, Germany).
Upper lid injections can be carried out using either a needle or cannula; however, the author’s preference is a needle. Topical anesthetic is applied. It is important to remember that the goal is not to try and fill the “black hole” of the hollow sulcus. This will likely consume a large quantity of filler, and in the end will not be successful. Instead, the HA filler is placed superficially with the goal to “unfold” the upper lid. The brow is elevated with one hand, and the first injection is at the level of the superior rim. Progressive injections are carried out, moving inferiorly each time. At a certain point, the infolded upper lid (representing the hollow sulcus) will pop out and become the more familiar and recognizable lid fold. At this point additional volumizing of the fold can be carried out with more filler in the areas where it is needed. Due to the extremely thin upper lid skin, small HA volumes are usually sufficient to achieve a good fold. Patients experience a “wow” factor when looking in the mirror even after only the initial injection. In some patients, either due to the thin eyelid skin, or a very deep sulcus, an initial volume of HA can be placed, and then the patient can return for further injections in 2 to 3 weeks. This allows the filler to settle, and the expanse of time between injections allows some volume augmentation by natural swelling of the HA. Vigorous massage over the superior rim is carried out by the injector, and the patient can apply cold compresses at home.
This technique is very useful for filling a hollow sulcus. In addition, it will also have an effect on the height and appearance of the crease ( Fig. 2 ). It is especially useful in cases of overaggressive upper blepharoplasty in order to correct the hollow as well as the increased TPS ( Fig. 3 ). Sometimes, HA filler to the upper lid may be combined with ptosis repair if indicated. As in the lower lid, HA filler tends to last a long time in the upper lids. Small touch-ups may not be necessary for quite some time after the initial injection ( Figs. 4 and 5 ).