Lower Lid Ectropion (Senile or Paralytic)
Description
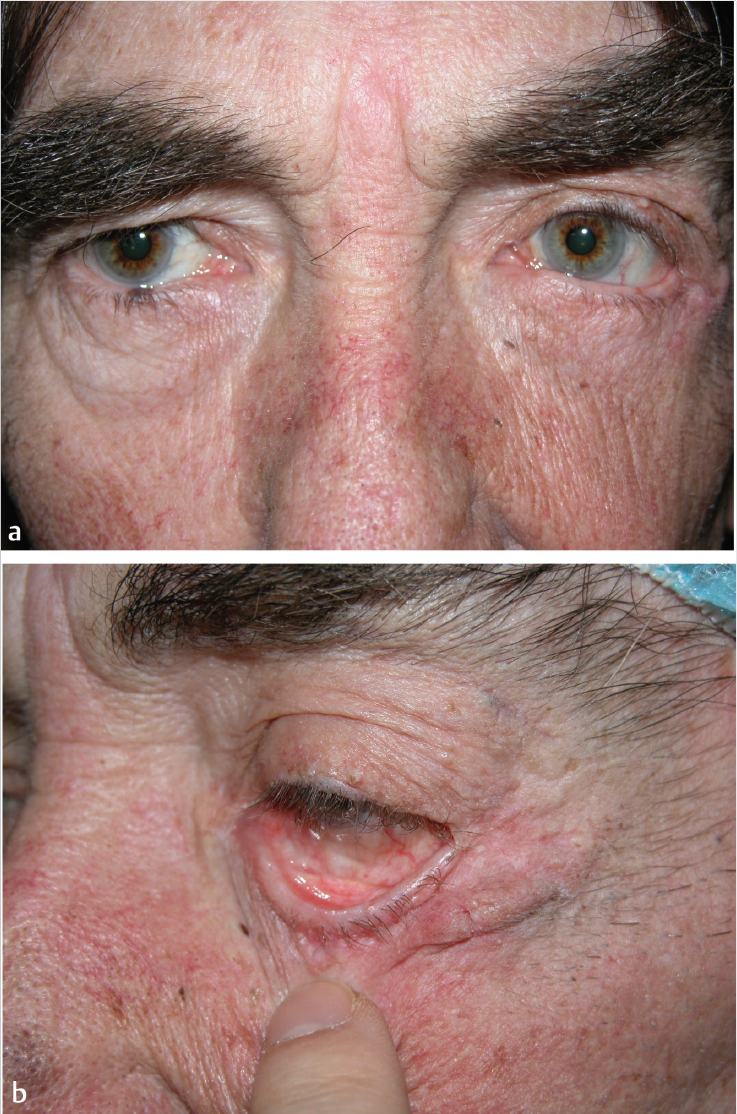
Lower lid ectropion: Outward turning of eyelid margin; involutional or senile caused by horizontal lid laxity and age-related weakness of the canthal ligaments and pretarsal orbicularis oculi.
Additional findings include upper eyelid laxity, brow ptosis (right more than left), and mild tear trough deformity of the right lower lid.
Work-up
History
Symptoms: Epiphora (excessive tearing), ocular irritation, xerophthalmia (dry eyes), poor cosmesis.
Classification: Punctal ectropion (lacrimal punctum everted only), medial ectropion, generalized ectropion, lagophthalmos (inability to completely close eyes), secondary exposure keratopathy, senile ectropion, paralytic ectropion, or cicatricial ectropion.
Physical examination
Snap-back test: Pull lower lid down and away from the globe for several seconds and wait. The eyelid should snap back immediately. Delay or inability to do so (without blinking) indicates significant ectropion.
Pinch test: Lid laxity is present if the lower eyelid can be pulled more than 6 mm away from the globe.
Medial canthal laxity test: Pull lower lid laterally away from the medial canthus and measure displacement of medial punctum; the greater the distance measured, the greater the laxity. Normal displacement is 0 to 1 mm.
Lateral canthal laxity test: Pull the lower lid medially away from lateral canthus and measure displacement of the lateral canthal corner; the greater the distance measured, the greater the laxity. Normal displacement is 0 to 2 mm.
Bell′s phenomenon: The patient attempts to close the eyes while the examiner holds the eyelids open. If the eyes rotate superiorly Bell′s phenomenon is present and indicates that this protective mechanism is in place.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


