Facial Paralysis

Description
Complete left-sided facial paralysis.
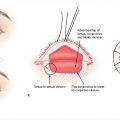
Facial asymmetry: Left palpebral fissure widening, left nasolabial fold effacement, right-sided deviation of Cupid′s bow, and inferior malposition of the left oral commissure, which demonstrates no movement with smiling.
The child has a fairly balanced brow position and minimal external nasal valve asymmetry.
Work-up
History
Onset of symptoms
Congenital or acquired.
Acute, subacute, or chronic.
Duration and rate of progression.
Complete or incomplete; unilateral or bilateral.
Associated syndromes or syndromic features.
Associated symptoms: Headaches, blurred vision, dry eyes, vertigo, hearing loss, otorrhea, oral incompetence, speech difficulties, snoring, nasal obstruction.
History of the following: Trauma; infection (Bell palsy, Ramsay Hunt syndrome, Lyme disease, tuberculosis); neuromuscular disease (myasthenia gravis, Charcot-Marie-Tooth disease, Guillain–Barré syndrome); tumors (neurofibromatosis type 2); diabetes; travel history; pregnancy; family history; surgical history (otologic, rhytidectomy, parotidectomy).
Physical examination
Perform complete head, neck, and cranial nerve examination.
Examine all branches of the facial nerve.
Temporal (frontal): Elevation of forehead.
Zygomatic: Closure of orbicularis oculi.
Buccal: Elevation of cheek and oral commissure.
Marginal mandibular: Depression of oral commissure and lower lip.
Cervical: Contraction of platysma.
Eyes: Evaluate eye closure, vision, corneal defects, ectropion.
Schirmer test (see Case 18).
Bell’s phenomenon (see Case 18): If absent, greater concern for corneal injury.
Evaluate facial movements at rest and in multiple different expressions.
Assess midline deviation, measure amount of excursion with movement.
Assess brow movement, nasal valve function, and synkinesis (involuntary contraction of additional facial muscles with voluntary facial movement due to aberrant neuroregeneration).
Assess overall muscle status (hypertonic, normal, or atrophic), voluntary and involuntary movements (synkinesis, fasciculations).
Pertinent imaging or diagnostic studies
Vary by case.
Hematologic work up: Complete blood cell count (evaluate for infection, leukemia), Lyme titer.
Temporal bone computed tomography.
Magnetic resonance imaging: To evaluate brain, facial nerve, or parotid glands.
Biopsy: Facial nerve, lip (for salivary tumors), fine needle aspiration of parotid mass.
Electrodiagnostic studies: Nerve conduction studies, electromyography (EMG).
Electroneurography (ENoG): Compares amplitude of summation potentials of paralyzed side of face with that of normal side.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


