Lower Lid Ectropion (Cicatricial)
Description
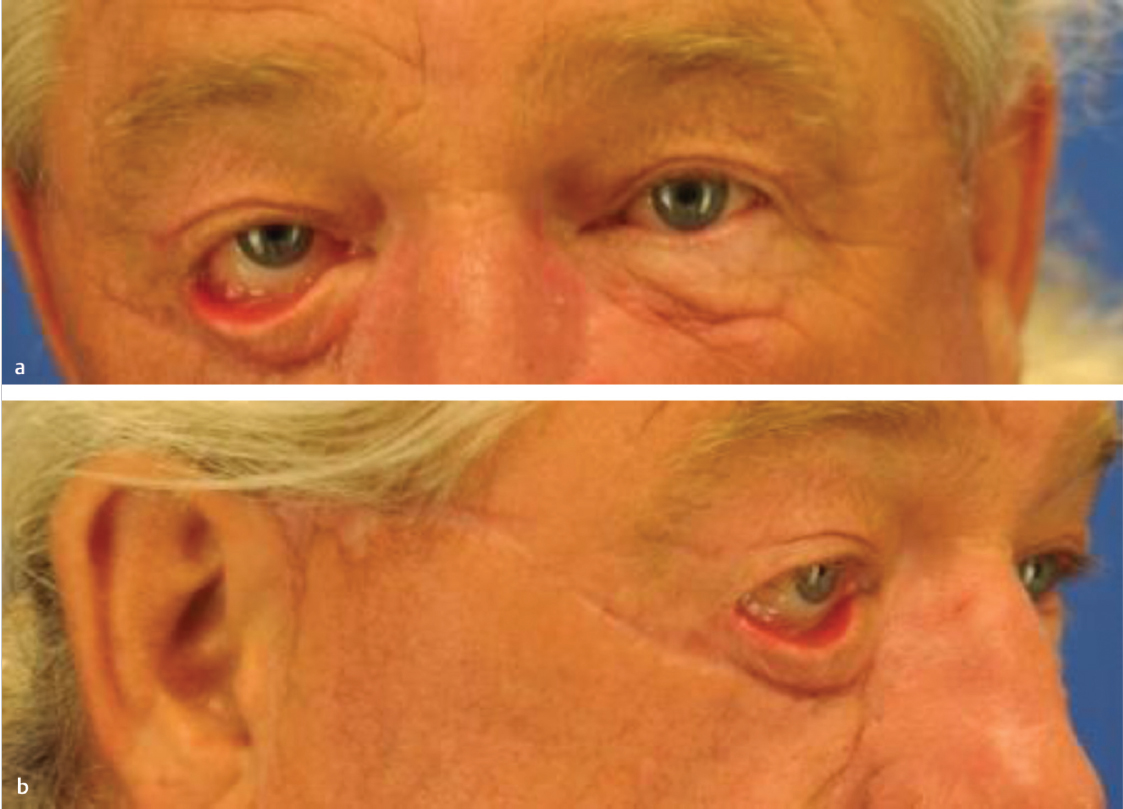
Lower lid ectropion: Eversion of the lower eyelid margin, resulting in scleral show and exposure of the conjunctiva.
Subciliary scar of the lower eyelid from previous operative procedure → cicatricial ectropion.
Background
Ectropion is the most frequent lid malposition seen clinically.
Characterized by eversion (outward turning) of the lid margin with exposure of the conjunctiva.
Classified according to time of onset and pathophysiology (cicatricial, senile, paralytic, congenital).
Cicatricial ectropion results from shortening of the anterior lamella of the eyelid.
Secondary to trauma, burn injuries, complications of blepharoplasty, involutional patterns, and medications.
Work-up
History
Symptoms: Epiphora (excessive tearing), ocular irritation, xerophthalmia (dry eyes), poor cosmesis.
Any prior eyelid-related surgeries or trauma. History of duration and progression of symptoms.
Ask about patient medications and if any new medications have been started.
Physical examination
Inspect the eye and lid margin. Evaluate location of the punctum.
The normal punctum position is inverted toward the lacrimal lake.
Evaluate for scleral show and rounding of the lateral canthus.
Epiphora: Excessive tearing due to punctum eversion.
Assess condition of the lower lid skin and support of the lower eyelid.
Evaluate for incomplete eyelid closure and corneal abrasions
Snap-back test: Pull lower lid down and away from the globe for several seconds and wait. The eyelid should snap back immediately. Delay or inability to do so (without blinking) indicates significant ectropion.
Pinch test: Significant lid laxity is present if the lower eyelid can be pulled more than 6 mm away from the globe.
Facial nerve function: Confirm function of orbicularis oculi to close eyes.
Bell′s phenomenon
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


