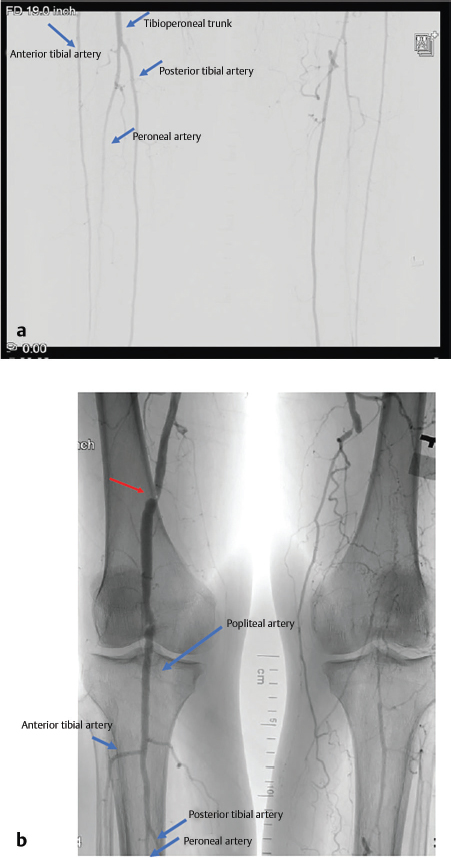
19 Lower Extremity Reconstruction Abstract This chapter will review the principles of lower extremity reconstruction after trauma. It will review preoperative assessment of blood flow and zone of injury, as well as reconstructive options. The readers will be able to analyze a given lower extremity injury and determine an appropriate operative intervention, and integrate the free flap failure algorithm in the management of postoperative complications. Keywords: lower extremity reconstruction, zone of injury Six Key Points • Determine the etiology of the wound. • Always assess the zone of injury. • Determine baseline function and neurovascular status prior to reconstruction. • Vascular integrity is key to lower extremity reconstruction. • Post-operative rehabilitation protocols are key to a successful outcome • Realistic expectations must be set for outcomes. A patient presents with an open leg wound after a motor vehicle crash. There is visible soft tissue loss. 1. What do you do? The injury is at least Gustilo 3b injury, which can be identified by the size of the defect (> 1 cm) and periosteal stripping, which leaves the bone exposed. If there is associated arterial injury, the classification is a 3c injury. This classification is useful because type III injuries require flap coverage of bone (Table 19.1). 2. What do you do? Assuming the patient is otherwise stable and orthopaedic surgery has adequately fixed the bone, preparations should be made for coverage. This begins with a full lower extremity examination, including motor and sensory function, and palpation of pulses. Imaging is then ordered. An angiogram is ordered. 3. The angiogram is shown in Fig. 19.1. Describe what is in the angiogram. The first vessel to come off of the popliteal artery is the anterior tibial artery, which appears the most lateral. The popliteal continues as the tibioperoneal trunk, and the next vessel, which appears medial to the anterior tibial artery, is the peroneal artery. The vessel then continues as the posterior tibial artery. 4. If only the posterior tibial vessel is open, what do you do? In that case, the case is more complex, but an end-to-side anastomosis can be performed. Table 19.1 Gustilo’s and Anderson’s classification of open tibial fractures
Questions
Case 1
Gustilo type | Description |
I | Wound < 1cm, no deep contamination |
II | 10 cm > wound > 1 cm without extensive soft-tissue damage |
IIIA | Wound > 10 cm with soft-tissue coverage of bone |
IIIB | Wound > 1 cm with exposed bone and periosteal stripping |
IIIC | IIIB with arterial injury |