Introduction
In this chapter we present the topic of reconstruction of soft tissue and bone defects in the lower extremity. We present the multiple indications for lower extremity reconstruction and review the decision-making process for proceeding with limb amputation versus salvage for cases of severe lower extremity trauma or major oncologic resection. We also discuss the likely postoperative sequelae and secondary challenges that arise after major limb reconstruction and we discuss the importance of a multidisciplinary approach for specific aspects of lower extremity patient care. The ultimate goal of lower extremity reconstruction is a functional restoration. The fundamental objectives for reconstructing a functioning motor unit are achieving durable weightbearing bony support, restoring stable and durable soft tissue coverage, and achieving pain-free mobility.
Preoperative Considerations
The etiology and level of defect must be considered during lower extremity reconstruction because these two factors will determine the surgical options available, probable time course for reconstruction, adjunctive treatment measures, possible complications, and rehabilitative expectations.
Etiology of Defect
The etiologies of major soft tissue or bone defects in the lower extremity are traumatic, infectious, oncologic, diabetic, vascular, or lymphatic. Traumatic injuries, necrotizing soft tissue infections, and oncologic resections account for most acute wounds. Diabetes, vascular disease, and lymphedema lead to chronic wounds ( Table 22.1 ).
| Acute | Chronic |
|---|---|
| Trauma | Diabetes |
| Oncologic resection | Peripheral vascular occlusive disease |
| Necrotizing soft tissue infection | Lymphedema |
Traumatic
Trauma is the most common etiology for lower extremity reconstruction. This is a well-studied topic with a wealth of literature on indications for reconstruction, treatment approaches, and outcomes. The mechanisms of these injuries vary according to region but may include motorcycle, motor vehicle, industrial, ballistic, and military trauma. In the practice of the senior author, the trauma demographic has an average age of 37 years, with a 2 : 1 male to female preponderance, and the mechanism of injury being mostly due to motorcycle or motor vehicle accidents. The severity of these injuries threatens the functional viability of the injured limb, and the surgical team must often decide whether to attempt salvage or perform amputation.
The trauma surgical team typically performs trauma triage and stabilization of life-threatening injuries according to advanced cardiac life support (ACLS) and advanced trauma life support (ATLS) guidelines. When major limb injury is apparent, specialties, including orthopedic surgery and plastic surgery, will join in a multidisciplinary effort. The trauma surgical team records the injury severity score (ISS) for all trauma patients, and they also apply the Mangled Extremity Severity Score (MESS) and Nerve Injury/Ischemia/Soft Tissue/Skeletal Injury/Shock/Age (NISSSA) scoring systems for extremity trauma ( Tables 22.2–22.4 ).
| The Injury Severity Score (ISS) is an anatomic scoring system that provides an overall score for patients with multiple injuries. Each injury is assigned an Abbreviated Injury Scale (AIS) score (see below) for each of six body regions (Head, Face, Chest, Abdomen, Extremities (including Pelvis), External). The highest AIS score in each body region is used. Each numeric score from the three most severely injured body regions is squared. The 3 squared numbers are added to produce the ISS. | |||
| Region | Injury description | AIS | (AIS) |
| Head and Neck | |||
| Face | |||
| Chest | |||
| Abdomen | |||
| Extremity | |||
| External | |||
| Injury Severity Score = Sum of 3 highest (AIS) numbers : | |||
| Abbreviated Injury Scale (AIS), 1990 version | |||
| AIS score | Injury | ||
| 1 | Minor | ||
| 2 | Moderate | ||
| 3 | Serious | ||
| 4 | Severe | ||
| 5 | Critical | ||
| 6 | Unsurvivable | ||
| Variable | Points |
|---|---|
| Skeletal/soft tissue injury | |
| Low energy (stab; simple fracture; civilian GSW) | 1 |
| Medium energy (open or multiple fracture, dislocation) | 2 |
| High energy (close-range shotgun or military GSW, crush injury) | 3 |
| Very high energy (above criteria + gross contamination, soft tissue avulsion) | 4 |
| Limb ischemia | |
| Pulse reduced or absent but normal perfusion | 1 * |
| Pulseless, paresthesias, diminished capillary refill | 2 * |
| Cool, paralyzed, insensate, numb | 3 * |
| Shock | |
| Systolic BP always >90 mmHg | 0 |
| Transient hypotension | 1 |
| Persistent hypotension | 2 |
| Age | |
| <30 | 0 |
| 30–50 | 1 |
| >50 | 2 |
| Type of injury | Degree of injury | Points | Description |
|---|---|---|---|
| Nerve Injury (N) | Sensate | 0 | No major nerve injury |
| Dorsal | 1 | Deep or superficial peroneal nerve, femoral nerve injury | |
| Plantar partial | 2 | Tibial nerve injury a | |
| Plantar complete | 3 | Sciatic nerve injury a | |
| Ischemia (I) | None | 0 | Good to fair pulses, no ischemia |
| Mild | 1 b | Reduced pulses, prolonged capillary refill, Doppler pulses present | |
| Moderate | 2 b | No pulses, prolonged capillary refill, Doppler pulses present | |
| Severe | 3 b | Pulseless, cool, ischemic, no Doppler pulses | |
| Soft tissue/contamination (S) | Low | 0 | Minimal to no soft tissue contusion, no contamination (Gustilo type 1) |
| Medium | 1 | Moderate soft tissue injury, low-velocity gunshot wound, moderate contamination, minimal crush (Gustilo type II) | |
| High | 2 | Moderate crush, degloving, high-velocity gunshot wound, moderate soft tissue injury, may require soft tissue flap, considerable contamination | |
| Severe | 3 | Massive crush, farm injury, severe degloving, severe contamination, requires soft tissue flap (Gustilo type IIIB) | |
| Skeletal | Low energy | 0 | Spiral fracture, oblique fracture, no or minimal displacement |
| Medium energy | 1 | Transverse fracture, minimal comminution, small-caliber gunshot wound | |
| High energy | 2 | Moderate displacement, moderate comminution, high-velocity gunshot wound, butterfly fragments | |
| Shock (S) | Normotensive | 0 | Blood pressure normal, always >90 mmHg systolic |
| Transient hypotension | 1 | Transient hypotension in field or emergency center | |
| Persistent hypotension | 2 | Persistent hypotension despite fluids | |
| Age (A) | Young | 0 | <30 years |
| Middle | 1 | 30–50 years | |
| Old | 2 | >50 years |
a Nerve injury as assessed primarily in the emergency room.
Trauma management during the modern military conflicts, including the Persian Gulf theaters, has enhanced our insight into management of the extremity trauma patient. Frequently in combat settings, damage control surgery becomes the essential strategy for catastrophic trauma victims. Approximately 21.4% of combat extremity trauma presents with life-threatening injury as compared with 10–17% seen in civilian trauma. The mechanism of injury is also different. Blast and penetrating missiles cause 79–90% of combat trauma, while blunt force accounts for the majority of civilian trauma. The trauma surgical team’s first priority in both military and civilian trauma is life-saving resuscitation, while limb reconstructive surgery is deferred until overall systemic stabilization is achieved. In settings where there may be delayed presentation to a medical facility, patients may begin to exhibit the “lethal triad” (pH <7.2; coagulopathy of INR >1.6; hypothermia of <34°C) as a consequence of the severity of their injuries. Their clinical condition evolves into a vicious deteriorating cycle if not properly managed. Without aggressive intervention, these patients may progress to metabolic failure, multiple organ failure, and systemic shock, which may ultimately prove lethal. In the scenario of impending development of the lethal triad, the surgical objectives for the extremity should be hemostasis and debridement. If there is a MESS score of ≥10 in this type of critical setting, limb amputation should generally be performed immediately. This type of patient frequently requires major trauma surgical intervention (such as thoracic or abdominal procedures), and the goal from the extremity salvage surgeon’s perspective is to participate productively with the trauma surgical team in a manner that limits the overall surgical time to <6 h. The acute care period will necessarily involve a critical care unit for systemic stabilization and treatment of acidosis, coagulopathy, and hypothermia. Subsequent wound debridement and reconstruction are performed at a time point determined by multidisciplinary discussion and agreement. During the acute period, compartment syndrome may also be evolving secondary to edema from the large area of muscular crush, bleeding into a contained fascia compartment, or from post-reperfusion edema in cases where muscle ischemia has exceeded 2 hours. Treatment teams must also be aware of the possibility of rhabdomyolysis whenever there has been a large volume of muscular crush. The treating team should monitor for this condition by checking blood levels of creatine kinase and potassium with specific attention to ample intravenous resuscitation and possible renal failure. Fat embolization is another potentially associated life-threatening condition, and any deterioration in respiratory status should trigger consideration of this possibility.
Oncologic
Major oncologic lower extremity reconstructions are mostly musculoskeletal in origin, and they are relatively less common. In some situations there needs to be a delay in reconstruction from the time of resection until the final histopathologic tumor margins are known. In such cases of delayed reconstruction, the brief initial period of the inflammatory healing process will obscure the tissue planes and potential recipient vessels to some degree, making reconstruction more challenging. Extremity sarcoma cases will frequently undergo preoperative neoadjuvant chemotherapy or radiotherapy. Both of these treatment modalities have a negative effect on healing capacity, and most surgeons wait 3–6 weeks from the last treatment before proceeding with definitive surgical resection and reconstruction to allow for adequate recovery of the patient’s inflammatory/wound healing capacity. Furthermore, the reconstructive surgeon should bear in mind that any previously irradiated field will have fibrotic tissue planes and friable recipient vessels that will also make reconstruction more challenging. The reconstructive measures taken for oncologic resections must provide an expeditious recovery, as adjuvant radiation or chemotherapy, which is critical to local control of the cancer, is usually postponed until definitive healing has occurred. This group of patients cannot afford to have a delayed course to adjuvant therapy due to prolonged wound healing.
Diabetic, Vascular, or Lymphatic Etiology
These patient groups are predisposed to ultimate reconstructive failure because of the tendency of wound recurrence due to the ongoing process of the systemic condition. The surgeon must bear in mind that undertaking major reconstruction within these clinical contexts without an attempt to substantially improve the systemic condition that is the root cause of the problem (e.g., major lifestyle alteration for diabetics, successful vascular surgical intervention, or successful vascularized lymph node transfer) is destined for failure. The operative prerequisites for diabetics should be stringent blood sugar control as measured by hemoglobin A 1C <7%, fitting for specialized orthotic diabetic shoes, and frequent podiatric monitoring. Patients with peripheral vascular disease (ankle brachial index of <0.7, toe blood pressure <40 mmHg, or transcutaneous oxygen tension [TcPO 2 ] levels <30 mmHg), must have undergone revascularization by the vascular surgery team prior to undergoing any major soft tissue reconstruction. Patients with lymphedema should receive intervention for the primary problem such as aggressive edema management measures, lymphatic reconstruction, or vascularized lymph node transfer, prior to soft tissue reconstruction.
Infectious Post-Debridement
Soft tissue defects resulting from debridement for infection are often associated with one of the aforementioned systemic conditions (diabetes, peripheral vascular occlusive disease, or lymphedema). Necrotizing fasciitis or Fournier’s gangrene will also lead to large skin defects that usually require skin grafting. Occasionally, exposed vessels, tendon, or bone will necessitate soft tissue reconstructions that are based on the same basic reconstructive principles detailed later. In the post-infection setting, attention to bacteriology will optimize the chances for success. Skin grafting should generally be delayed until bacterial quantities are <10 8 organisms/g of sampled tissue. Furthermore, the presence of beta-hemolytic streptococci and Pseudomonas in any quantity has been observed to have a detrimental effect on skin graft success. Involvement of an infectious disease specialist for a well-directed antibiotic regimen is also advisable.
Level of Defect
The level of defect dictates what reconstructive options are available. The distal one-third level is traditionally held as the critical boundary, beyond which local or regional flap reconstructive options do not exist and microvascular free tissue transfer becomes mandatory. However, with the advent of perforator-based pedicled fasciocutaneous flaps, relatively smaller distal one-third defects often no longer require free tissue transfer. However, larger defects in the distal one-third leg or foot still frequently need free flap coverage.
Indications
Traumatic Indications for Surgery
Salvage Versus Amputation
The context of reconstruction of the traumatized lower limb should be understood by considering the approach to the most severely injured patient. In this scenario, the decision for limb salvage versus amputation proceeds by first classifying the patient according to the following three categories. One group of patients presents with severe limb injury and concomitant life-threatening conditions, and limb salvage is incompatible or significantly risky for life preservation. These patients should undergo amputation. A second group of patients presents with severe limb injury and no imminent life-threatening injuries. In these patients, sensation and distal mobility is preserved, and limb salvage is attempted. However, the most challenging treatment category of patients is the third group, who present with severely damaged and de-functionalized limbs whose functional prognosis is uncertain. For these patients falling into the “gray zone,” a wealth of outcomes-oriented investigation over the last two decades has sought to provide reliable guidance on the decision for amputation versus limb salvage. Multiple scoring systems have been devised, including the Predictive Salvage Index (PSI); Mangled Extremity Severity Score (MESS); Limb Salvage Index (LSI); Hannover Fracture Scale; and the Nerve Injury/Ischemia/Soft Tissue/Skeletal Injury/Shock/Age (NISSSA) score. Subsequent studies including the Lower Extremity Assessment Project (LEAP) series assessed these scoring systems and tried to define the characteristics of the individuals who sustained these injuries, the characteristics of their environment, the variables of the physical aspects of their injury, the secondary medical and mental conditions that arose from their injury and treatment, their ultimate functional status, and their general health. Furthermore, these investigations analyzed complications and instances of secondary amputation, and none of the lower extremity injury severity scoring systems could be consistently validated for deciding on amputation versus salvage. The source of the disagreement may be due to the highly variable patient population of different regions, and the different personal factors that substantially affect life outcome after such catastrophic injury. Our group has generally been able to achieve worthwhile functional reconstructions and patient satisfaction for MESS <10. If MESS is ≥10, we generally recommend amputation but ultimately allow the patient and family to decide. Our reconstructive goals are to provide functional restoration by combining a competent weightbearing bony support with a functional motor unit, to yield a stable, durable, and pain-free limb. There is some evidence that limb salvage is psychologically beneficial even when functional outcome may not be better than prosthetic replacement. Since very few limbs in the clinically stable patient are not primarily salvageable with the current arsenal of reconstructive modalities, our goal is to have the patient arrive at an informed treatment decision after a reasonable consideration of the relevant factors of overall patient health, expected functional recovery of the salvaged limb versus expected prosthetic functional level, and socioeconomic circumstances (ability to take time away from work and available support network at home); it should be noted that there is an association between favorable functional outcome and adequate family help, as shown in the LEAP study. Surgery should be pursued only after careful consideration of these factors in the context of each individual patient.
Traumatic indications for reconstruction generally involve restoration of one or more of the following components: bone, nerve, vasculature, muscle, tendon, and soft tissue cover. After initial stabilization, the surgical team will then make an accurate anatomic catalog of injury to allow for a systematic decision-making process upon salvage versus amputation. Vascular anatomy should also be noted from the standpoint of whether tissues distal to the injury are viable and which of the three branch vascular runoff is preserved, as this will affect planning of potential microsurgical reconstruction. The extent of bony destruction should be considered in regard to whether internal or external fixation alone may be expected to provide bony integrity or if vascularized osseous tissue will be needed. Assessment for nerve injury by meticulous sensory and motor exam should determine the precise location of suspected nerve injury at the sciatic, tibial, deep peroneal, or superficial peroneal levels. With open injuries, nerve integrity often will have to be definitively assessed intraoperatively by visualization. It should be noted that an insensate foot upon initial presentation is no longer a criterion for amputation given the frequency of recovery of function. The musculotendinous units that have been violated by injury should be noted with particular attention to what possible functional restoration may be attempted in a concomitant effort to provide the necessary soft tissue reconstruction.
Surgical Objectives in the Acute Setting
Vascular Integrity
Attention should be first directed toward verifying vascular integrity. Distal ischemia should always be first treated by a trial of reduction of bony fracture, which often will restore distal vascularity. Injury of at least one of the three vascular trunks will frequently be present in the majority of Gustilo IIIB or IIIC injuries, and CT angiography is a low morbidity study that should be performed for both the purposes of assessing a need for vascular repair and also choosing the appropriate recipient site and technique (end-to-side vs end-to-end) for microsurgical reconstruction. If distal ischemia has been ongoing, the plan for surgical intervention should involve an immediate reestablishment of vascular inflow by placement of a temporary vascular shunt. An assessment of vessel defect should determine the potential need for vein grafting. Our group’s preferred technique for vein grafting of greater length involves the temporary creation of an AV fistula. Vessel defects requiring vein graft reconstruction will require a concomitant overlying soft tissue reconstruction. Recipient vessel selection should be considered at this time. Our group’s preference is to perform end-to-end anastomoses adjacent to the injured area, choosing a vessel that shows no signs of injury (lack of vigorous flow, thrombus, avulsed branches, intimal tearing, “ribbon” sign). If a vessel is damaged, it still may be used in an end-to-end fashion, but it must be trimmed back to a healthy zone with a high degree of certainty and precision in order to achieve a high rate of flap viability. However, if all vessels are involved in the zone of injury and determined unsuitable, one should utilize a vein graft to a site proximal to the zone of injury in an end-to-side fashion. One may also consider the possibility of using the contralateral leg in a “cross-legged” free flap fashion. Our group’s preference for venous drainage of the flap is to use the deep venous systems whenever possible due to their proximity to the recipient artery and their decreased likelihood to be involved in a zone of injury.
Debridement and Timing of Soft Tissue Reconstruction
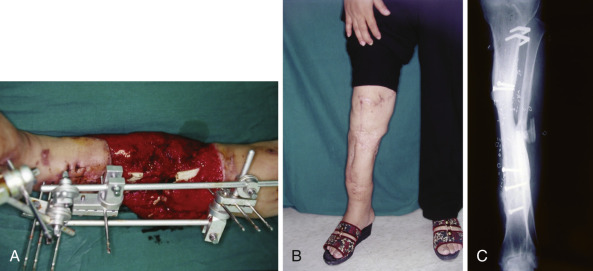
After salvage has been decided upon, attention to a thorough surgical debridement is paramount. Our group’s opinion echoes many other centers in that surgical debridement is critical to the ultimate success of the reconstruction. Inadequate debridement will ultimately result in infection, which may manifest as a persistent wound, osteomyelitis, bony non-union, or flap failure. Consideration of wound debridement lends naturally to the topic of timing of reconstruction. While previous studies have designated certain timeframes and suggested the importance of adhering to time restrictions in achieving wound coverage, more recent literature has arisen to counter this argument. Our feeling is that adequate surgical debridement should dictate the time course of reconstruction. For instance, a blast injury may necessitate repeated surgical debridement to achieve a healthy and clean wound bed. While there is a general effort to minimize the time to wound coverage, the overriding objective is to continue with surgical debridement until a healthy and viable wound bed is certain ( Fig. 22.1 ). Our group agrees with the recommendations of the EAST protocol with Gram-positive and Gram-negative coverage continuing for 72 h after injury and 24 h after soft tissue coverage. In the patient population discussed in this chapter (mutilating-type injuries often with extensive contamination), we have an extremely low threshold for broadening coverage to include anaerobic flora or extending treatment to 7–10 days after flap reconstruction.

Nerve Reconstruction
In mutilating lower extremity trauma, one must screen for concomitant nerve injury by an anatomic approach, as described earlier. One must precisely locate any suspected nerve lesion. Any vascular injury should automatically raise concern for concomitant nerve injury given the usual proximity of vessel location to nerves. Nerves should be explored at the time of surgery whenever there is sensory or motor deficit in the context of a large open injury and repaired primarily by nerve graft at the initial reconstruction if the mechanism is sharp. If the mechanism of injury is a crush or blast, nerve reconstruction should proceed in a delayed fashion. Sciatic lesions have the worst functional prognosis; realistic hopes for reinnervation should be limited to recovery of hamstring or calf muscle function and protective sensation at best. Tibial nerve injuries below the knee have a somewhat better prognosis with direct repairs and nerve grafting, yielding 39–62% sensory recovery and 27–79% motor restoration, as reported in previous literature. Common peroneal nerve transections have relatively the best expectation of recovery with direct repair and nerve grafting <6 cm yielding 84% and 75% rates of successful recovery of motor and sensory function.
Bony Restoration
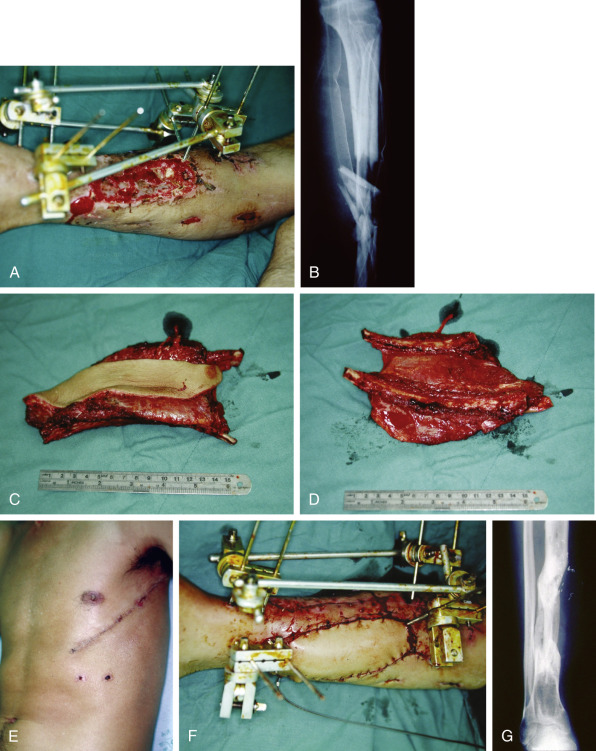
Mutilating lower extremity injuries often test the limit of orthopedic capability. Many of these injuries require either external fixation or procurement of additional vascularized bony tissue for reconstruction. Smaller bony defects up to 6 cm may be treated by conventional bone grafting at 6 weeks to minimize the risk of infection. Bony defects of the tibia and femur exceeding 6 cm in length are best treated by single-stage vascularized osseous flap transfers. Reconstructions of ≤10–12 cm may be achieved with osteomusculocutaneous flaps harvested from the fibula, rib-serratus anterior, or iliac crest-groin flap donor sites. The potential donor site morbidity with fibula harvest (great toe dysfunction, skin graft failure, ankle pain) is generally more minor that that of iliac crest or rib harvest, which may incur abdominal hernia and pneumothorax, respectively. If using the rib-serratus anterior composite flap in situations such as with bilateral tibia-fibula fractures when the fibula is unavailable, we typically harvest a pair of non-consecutive ribs to allow for a “double-barrel” design that provides better structural stability. The fibula osteocutaneous flap is the preferred technique for bone defects up to 18 cm and their associated soft tissue requirements, as it has been shown to provide the greatest amount of cortical bone and also to have the lowest rate for surgical complications such as osteomyelitis, skin paddle partial loss, stress fracture, non-union, and secondary amputation. At the upper limits of bone requirement, it is occasionally necessary to rely on a single-strut reconstruction, and our group has found these reconstructions to evolve to excellent stability and durability with the excellent potential for bony hypertrophy that is present in vascularized bone. Of note, the fibula and rib donor sites seem to have a more rapid rate of hypertrophy than the iliac crest, but all three methods achieve comparable weightbearing capacity at 2 years postoperatively ( Figs 22.2–22.4 ). Some groups advocate a staged reconstructive process in situations of substantial concomitant bony and soft tissue defect. They recommend soft tissue coverage followed by vascularized bone graft at a later stage. However, this approach prolongs both the reconstructive timeline and the period of disability for the patient. Furthermore, during the surgery for the second free flap, the surgeon will encounter a fibrotic soft tissue environment around the recipient vessels that may render them unsuitable for use. Our group has demonstrated the ability to reliably perform one-stage composite soft tissue and bone reconstruction with similar functional outcomes to the staged approach. The average time to bony union in our series of osteocutaneous reconstruction was 8.5 months.

Soft Tissue Coverage
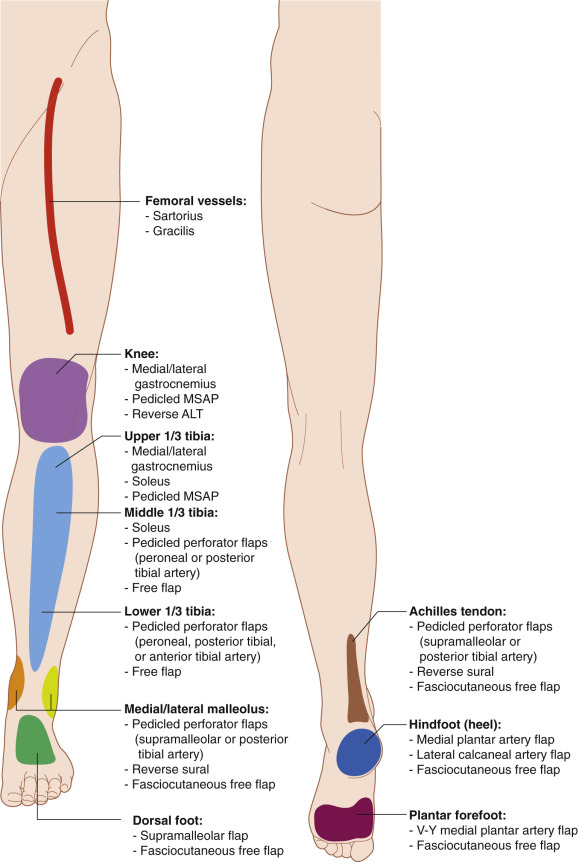
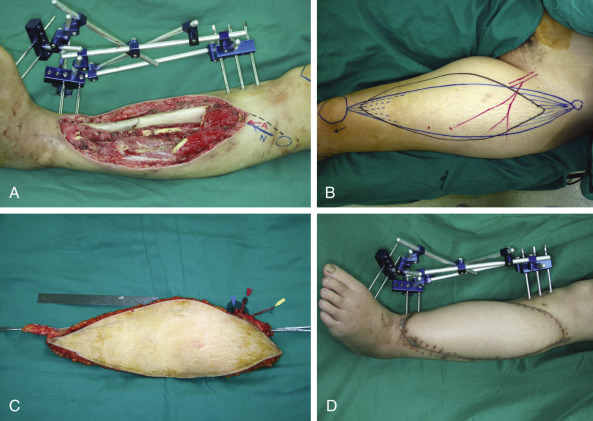
Traumatic lower extremity injury often creates a deficit of soft tissue. Soft tissue defects requiring reconstructive flaps will occur in the following areas: large vessels of the thigh, knee, tibia, Achilles tendon, medial malleolus, lateral malleolus, dorsal foot, hindfoot, and forefoot ( Fig. 22.5 ). The goals of reconstruction are to provide durable coverage of critical structures (healing bone, tendons, or vessels). Ideally, this initial reconstruction should be done in a manner that eliminates the need for future procedures whenever possible. Specifically, if an entire functional musculotendinous unit is sacrificed by the initial trauma, our group’s preference is to replace that musculotendinous unit at the initial stage of reconstruction with a functioning free muscle transplantation (FFMT). For instance, trauma that has caused irrecoverable functional loss of any one of the anterior compartments, posterior compartment, Achilles tendon, or patellar tendon in the leg may be reconstructed by an immediate single-stage composite rectus femoris FFMT with anterolateral thigh (ALT) flap skin paddle if necessary. Both flaps are based upon the lateral circumflex femoral artery system ( Fig. 22.6 ).
Secondary reconstructive requirements frequently arise, and thus the primary effort at soft tissue reconstruction should always be performed in a manner that facilitates possible second-stage procedures (e.g., flap re-contouring or tendon transfer). The preference of our group is to use microvascular transfer of fasciocutaneous tissue for defects around the metaphyseal regions of the knee and ankle since these flaps have been shown to be equally effective as free muscle flaps in preventing osteomyelitis and promoting bony union. Furthermore, these flaps provide soft tissue with a smooth, gliding undersurface that may be easily re-elevated because traumatic cases involving the joints will frequently require secondary procedures such as joint contracture release or tendon transfer. When there is a substantial 3-D soft tissue defect such as around diaphyseal fractures that require dead space obliteration, we use a myocutaneous flap.
Proceeding with Amputation but Preserving Length
Mutilating lower extremity trauma may result in a leg that has no potential for salvage, or amputation is chosen due to patient preference. In these situations it may become necessary to devise measures to preserve length on the residual leg as the morbidity of proximal amputations is far greater than of distal amputations. “Spare parts” from the amputated part should always be considered first as a source for tissue coverage, as with use of a fillet flap for proximal tibial coverage to allow for preservation of adequate proximal tibial length for pursuit of a below knee rather than above knee amputation prosthesis and better functional outcome.
Oncologic Indications
Oncologic reconstruction for the purpose of limb preservation was born from principles learned in trauma reconstruction. Thus, oncologic indications for surgery can be understood in an analogous framework, as with trauma. Just as in the trauma setting, the plastic surgery team is called upon to restore one or more of the following components that has been resected with the tumor: bone, tendon, nerve, vasculature, muscle, and soft tissue cover. The same general principles apply for deciding upon the reconstruction of each component. The great advantage of oncologic reconstruction is that the conditions are relatively more controlled. The defects of bone or soft tissue are far more predictable, as preoperative imaging or tissue biopsies allow for an approximate operative plan to be established. Nerve defects should be reconstructed immediately with nerve graft. Some oncologic cases necessitate immediate bony reconstruction with cadaveric or vascularized bone graft. There is a frequent need for postoperative radiotherapy in these instances. In these cases, we advocate the general approach of covering all hardware or cadaveric bone with a layer of healthy vascularized muscle to minimize the chance for major complications such as non-union, fracture, or hardware exposure. Of note, the development of hardware or cadaveric bone exposure in this setting is a limb-threatening condition with amputation rates as high as 50%. If the soft tissue deficit involves the entire muscle compartment eliminating an entire functional unit, our group prefers immediate reconstruction using functioning free muscle transplantation.
Diabetic, Vascular, or Lymphatic Indications
Defects in the lower extremity by these etiologies are usually deficits of soft tissue cover. Similar to the trauma setting, the chronic wound must be thoroughly debrided – all necrotic tissue (including bone) must be removed in order to allow for the possibility of successful reconstruction. Furthermore, wounds in these contexts may frequently necessitate consideration of adjuvant antibiotic treatment to maximize the chance of healing after resection of necrotic bone associated with osteomyelitis. Major defects involving musculotendinous units or bone resulting from attritional destruction by the chronic wound are rarely amenable to reconstruction and usually require some form of amputation due to the certain presence of extensive osteomyelitis.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


