Low-Volume Fat Grafting for Contour Correction
Nolan Karp
Jordan D. Frey
DEFINITION
The popularity of fat grafting to the breast has grown immensely since it was first described in the late 19th century with greater than 60% of plastic surgeons now utilizing fat grafting in reconstructive breast surgery.1,2
Autologous fat grafting has proven to be extremely efficacious in correcting volume and contour deformities both after postmastectomy breast reconstruction and after breastconserving therapy.1,3,4,5
ANATOMY
Contour deformities of the breast to be corrected with small-volume fat grafting may arise from a myriad of anatomical etiologies.
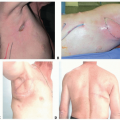
In implant-based breast reconstruction, the gentle slope of the natural superior chest wall-breast junction is often difficult to reconstruct, resulting in a superior shelf contour deformity.
Additional volume or contour abnormalities to be corrected may arise from size discrepancy between the implant and breast envelope or inadequate implant volume or due to complications of the initial reconstruction, such as mastectomy flap necrosis.6
In autologous breast reconstruction, irregularities requiring fat grafting may develop due to inadequately sized flaps secondary to donor site paucity as well as from flap complications, such as fat necrosis.6
Patients with small breasts or large tumors are particularly prone to contour irregularities that require fat grafting after breast-conserving therapy.3
Possible anatomical donor sites for small-volume fat grafting of the breast include the abdomen, flanks, lateral and medial thighs, back, and buttocks.5
PATIENT HISTORY AND PHYSICAL FINDINGS
The decision to proceed with fat grafting to the breast for contour correction after either breast reconstruction or breast-conserving therapy is based largely on physical examination and patient preference.
Patients should be followed at regular intervals after their initial breast reconstruction to evaluate for evolving breast volume asymmetries or contour irregularities.
In evaluating a subpectoral implant reconstruction, the breasts should be examined both statically and with pectoral contraction to observe for dynamic irregularities.
Patient expectations should be assessed prior to proceeding with fat grafting; patients should be made aware of any prereconstruction breast asymmetries that will not be changed by fat grafting.
Donor sites are chosen based on availability and patient preference to ensure that there is sufficient autologous fat to correct all breast deformities.8
IMAGING
Patient photography should be obtained after breast reconstruction and compared with preoperative photographs to help plan for contour correction with fat grafting.
Traditional radiographic imaging is typically not required prior to secondary breast reconstruction with small-volume fat grafting.
MRI may at times be helpful in assessing the volume required for adequate contour correction; there is a substantial added cost with this technology, however.
SURGICAL MANAGEMENT
Patients should wait a minimum of 3 to 4 months after their final implant placement, flap reconstruction, or breast-conserving procedure prior to proceeding with fat grafting for contour correction.
This will allow adequate time for tissues to heal and soften, both defining the final contour of the breast and increasing recipient bed vascularity.
In general, small-volume fat grafting of the breast is best accomplished under general anesthesia given the multiple areas of surgery and need for position changes.
Preoperative Planning
Physical examination, patient photography, and 3D imaging should be utilized preoperatively to precisely plan the location and amount of fat grafting required for adequate contour correction.9,10
Given the fluctuating nature of adipose deposits, potential donor sites should be reassessed on the day of surgery to plan the volume of autologous fat to be harvested from each site.
Positioning
Patient positioning in the operating room is dependent on the donor sites from which autologous fat will be obtained.
Patients should be positioned on a bed permitting flexion at the hips so that the patient may be able to “sit up” during the procedure.
A prone position with arms extended forward in a diver’s pose is necessary if the back or buttocks are to be harvested.
If required, the patient should begin in the prone position for autologous fat harvest prior to being placed in the supine position for additional fat harvest and recipient site grafting as indicated.
A supine position is planned if the abdominal, flank, or lateral and medial thigh donor sites are to be harvested.
These sites are advantageous as both donor site harvesting and recipient site fat injection can proceed without position change.
In the supine position, the arms should be abducted at approximately 90 degrees and secured to the arm boards in preparation for sitting the patient up during the procedure.
Approach
The donor site areas from which the autologous fat will be harvested should be marked with concentric circles. Recipient site areas into which the fat will be grafted should be marked with cross-hatches on the patient.
Markings for cannula access incisions should be placed in all donor and recipient sites within relaxed skin tension lines in areas typically hidden by clothing.
TECHNIQUES
▪ Tumescent Infiltration of Donor and Recipient Sites
Tumescent solution is prepared using 20 cc of 2% lidocaine, 1 mg of 1:1000 epinephrine within one liter of lactated Ringer solution.8
Lidocaine concentrations of 35 mg/kg have been proven safe using the tumescent technique.11
Planned 2-mm stab incisions near donor and recipient sites are made with an 11-blade while pinching the skin to avoid damage to deeper structures.
Tumescent solution is infiltrated using a tumescent cannula at rates ranging from 50 to 200 mL/min into all areas of autologous fat harvest as well as all planned recipient sites.11
The end point of tumescent infiltration is judged on the basis of tissue turgor and skin blanching and is generally in the ratio of 2:1 infiltrate to aspirate.11
Ideally, 15 to 20 minutes is allowed to elapse prior to liposuction fat harvesting to maximize the vasoconstrictive effect of the tumescent solution.12
▪ Donor Site Autologous Fat Harvesting With Liposuction
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


