Summary
Local flaps can provide immediate definitive wound closure but at the expense of distant incisions and increased repair complexity.
Although geometric flaps are well described and popular, the human face has no inherent right angle geometric patterns.
Simple linear closure frequently provides the best outcome and should always be considered.
9.1 General Considerations
The numerous classification systems for local flaps do not necessarily contribute to their clear understanding. Flaps may be classified by the native blood supply (random or axial pattern), the geometric configuration (i.e., rhombic, bilobed, trilobed), the location of either the defect or the pedicle (regional, pedicled), and by the method of transfer of the flap. The method of the transfer seems to provide the most clear representation of the flap and that will be utilized in this chapter. Three types of local flaps will be described: rotation, advancement, and transposition flaps. All of these flaps are confined to head and neck facial reconstruction.
The advantages of the local flaps are their ability to provide vascularized color- and texture-matched skin for reconstruction. The majority of the repairs can be done as a single stage. The disadvantages to local flaps are not trivial and include often extensive incisions distant from the site of the defect and the opportunity for wide and irreversible anatomic component distortion. The most obvious example of this is a poorly designed or executed bilobed flap that can irreversibly distort the nasal ala. Additionally, the consequences of a flap failure, all or partial, are not insignificant. The potential disaster for a complex local flap being performed in the case of an incompletely excised or recurrent skin cancer and the subsequent provisions that have to be made for cancer clearance after the formation and inset of a flap are tremendous. Appropriate planning for local flap reconstruction includes a very careful assessment of the defect, but more importantly the flap donor site. As an example, the limitations on use of a bilobed flap in nasal reconstruction are most dependent on the site of the secondary lobe and its subsequent closure and possible distortion of the lower eyelid versus the initial lobe placement. Appropriate reconstruction planning must always include alternatives to flap reconstruction and the placement of flap incisions, as they relate to any “lifeboat” provisions for a failed flap.
9.2 Linear Closure
Although not technically a local flap, simple linear closure constitutes the majority of nongraft repairs and merits discussion on proper execution.
The advantages include unmatched simplicity, reliability, and speed. Properly performed, it can yield the “best” result in all small and many large defects. Understand that ideal relaxed skin tension lines facilitate final incision placement. 1 Meticulous and complete standing cone or dog-ear excision is required, given that standing cone rarely “settles” completely. Skin undermining is rarely indicated and its benefit is overrated on inset, as it contributes to seroma or hematoma formation and devascularizes the inset.
For proper performance of linear closure, the surgeon will place a single silk tacking suture in the center, but 90 degrees from the estimated ideal closure orientation. The wound is tailor tacked closed and then the suture is now placed at the new best guess of the ideal closure orientation. Any retraction of anatomic features, especially eyelid, is evaluated. As a rule, any eyelid retraction or nasal alar retraction is a firm contraindication to linear closure, but mild lip retraction almost always resolves. The single central suture location is marked and the standing cones are marked for excision with surgical marker. The suture is removed and the standing cones meticulously excised. It is very important to conceptually understand that the standing cones must be excised to the depth of the central defect. This is not simply a skin-only excision, but rather a skin and soft-tissue debulking to result in a symmetric depth throughout the closure. The process is somewhat akin to “digging a ditch” with each end symmetric to the middle. Undermining is rarely required and meticulous linear closure to the level of the skin is performed. There really is no perceptible difference in final outcomes based on final skin closure techniques. As long as the skin is reached in closure with elimination of all deep dead space without any undue tension, any choice of skin closure can yield an equivalent result. 1 Other issues regarding skin closure can be considered, including surgeon’s preference, need for patient follow-up, as well as the patient’s preference. It seems prudent for the beginning surgeon to try a number of different skin closure techniques to determine what works best for his practice and patients (▶ Fig. 9.1, ▶ Fig. 9.2, ▶ Fig. 9.3).
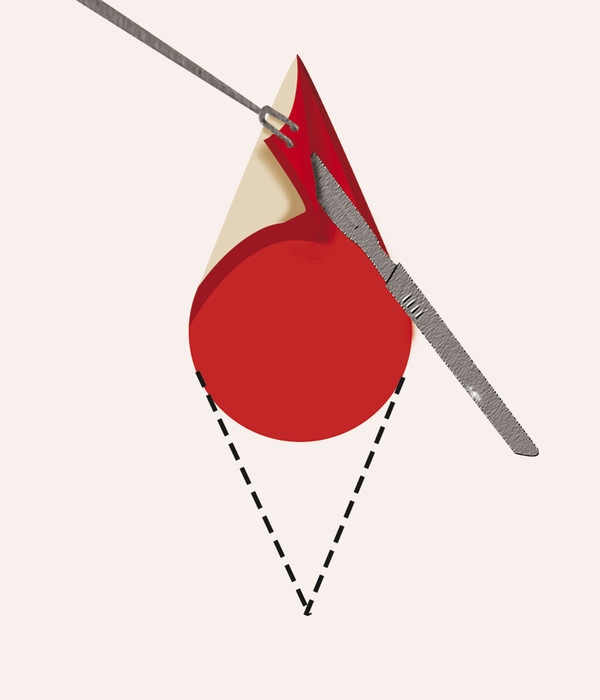
Fig. 9.1 Standing cones are meticulously excised. This includes skin and subcutaneous fat.
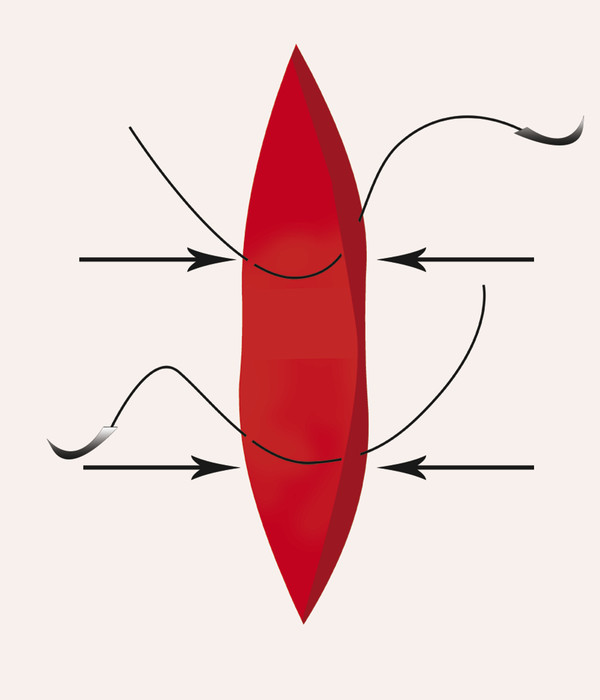
Fig. 9.2 When the depth of the wound is the same, deep load-bearing sutures are placed at the vertex of each dog-ear excision, avoiding deep sutures placed in the central, most tissue-deficient portion of the wound.
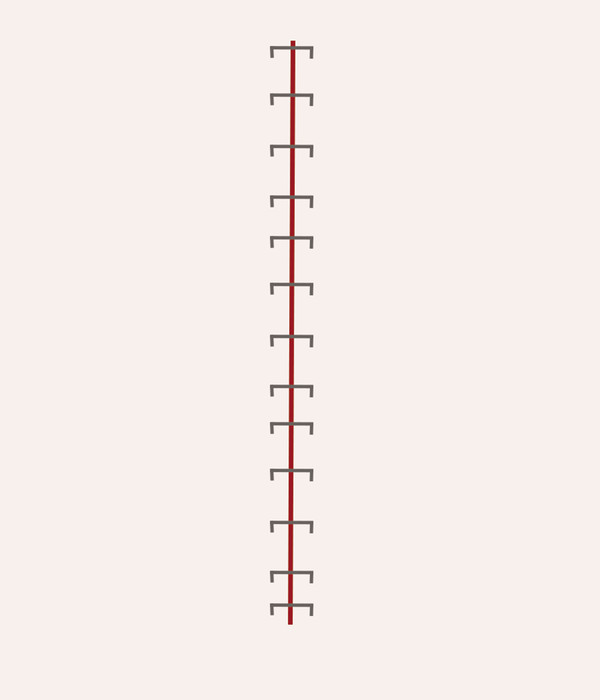
Fig. 9.3 A wide variety of skin closure techniques will yield similar results, as long as the final layer of closure is performed under little or no tension.
9.3 Rotation Flaps
Rotation flaps are a type of pivotal flap where the flap is designed so that the leading edge of the flap is also bordering the defect. They are the most commonly utilized, the most anatomically correct, and easiest to visualize. A rotation flap relies on the conversion of any defect into a triangular defect, where the base of the triangle forms a portion of the circumference of the flap arc rotation circle. 2, 3 The base of the flap then becomes the radius of the flap rotation circle and these flaps are very easily designed and executed, particularly on large flat featureless areas such as the scalp or the cheek. 2, 3 Two provisions to provide safe inset are caution in the back cut that cuts into the base of the flap at the consequence of decreased flap vascularity and a meticulous Burrow’s triangle which is required to eliminate the standing cone that arises from the mismatched flap radius (▶ Fig. 9.4, ▶ Fig. 9.5, ▶ Fig. 9.6, ▶ Fig. 9.7).
Fig. 9.4 The flap begins with conversion of defect to a triangular configuration so that base of triangle forms a portion of the flap circumference.
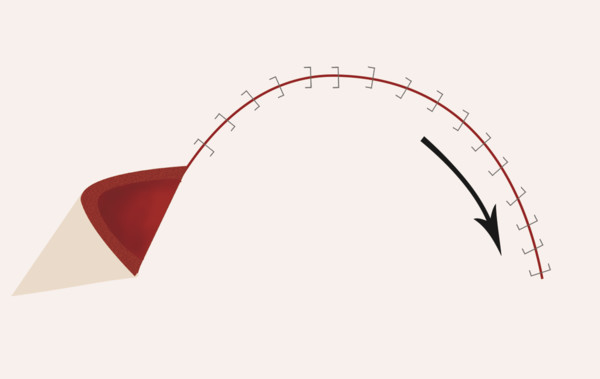
Fig. 9.5 As the flap rotates to fill the defect, a standing cone develops.
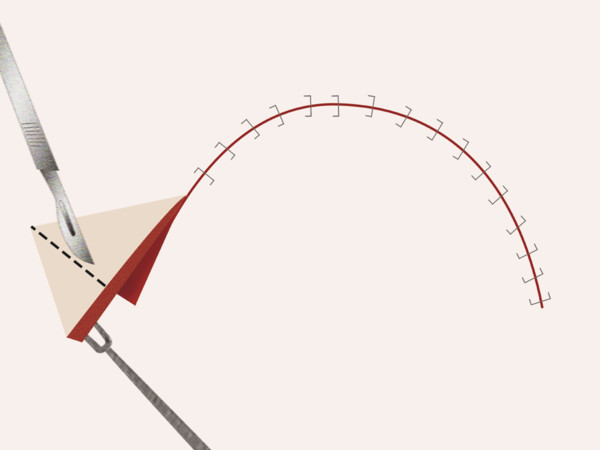
Fig. 9.6 A true Burow’s triangle excision of the standing cone is performed.
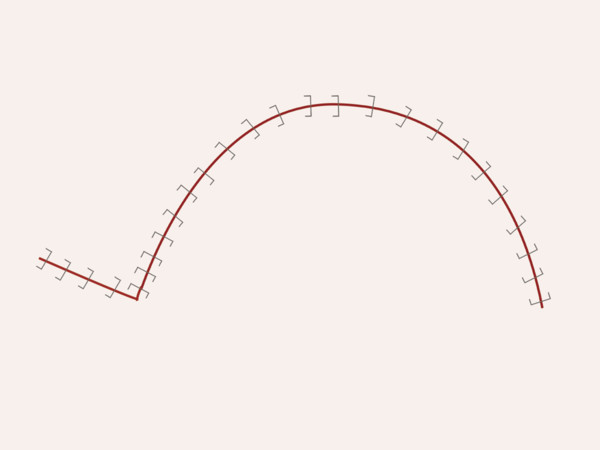
Fig. 9.7 Final flap inset.
9.4 Advancement Flaps
Advancement flaps are useful on featureless and flat areas, such as the cheek and scalp. One detractor is the required long linear incisions which ideally are placed within natural soft-tissue borders. The most common and useful example of advancement flaps is the V-Y advancement flap, where planned incisions can usually be placed within soft-tissue borders and ideal contour as well as color-matched skin and soft tissue can be advanced into the wound. If a V-Y advancement flap design includes a single perforator vessel identified by Doppler, the entire flap can be safely elevated on that single vessel. This allows for significant dissection up to the identified pedicle and permits generous and safe flap advancement.
During flap design, a single tacking suture can be placed within the defect and the leading edge of the planned V-Y advancement flap. If this closes, even with significant distortion, one can be assured that after flap elevation, there will be enough laxity to affect closure without distortion (▶ Fig. 9.8, ▶ Fig. 9.9, ▶ Fig. 9.10).
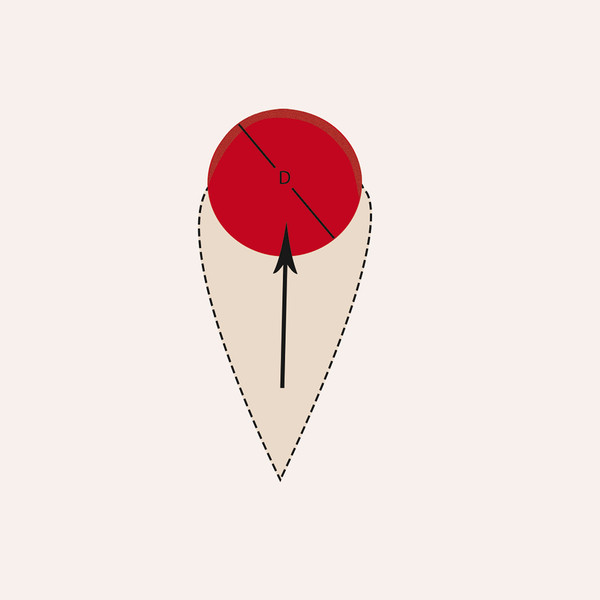
Fig. 9.8 The leading edge of the V-Y flap is designed slightly larger than the defect.

Fig. 9.9 The flap can be elevated and advanced based on a single arterial perforator.
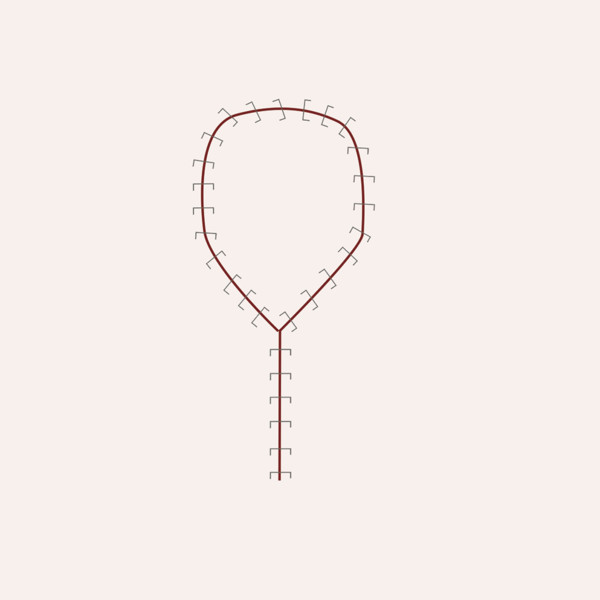
Fig. 9.10 Final flap inset.
9.5 Transposition Flaps
The last flap design is transposition flaps. Basically, a transposition flap is created where the donor site is remote from the defect and the flap is moved about the pedicle or transposed over intervening normal tissue and into the defect. It is a commonly used flap for head and neck reconstruction. We will discuss three examples of it. It provides the advantage of immediate flap inset of color-matched and texture-matched tissue with often a direct linear closure of the donor site. The difficulties of transposition flaps also involve obscuring natural contours or providing distortions at site distant to the defect. Two examples of these would be a melolabial transposition flap that distorts the contour of the cheek–nose junction or a poorly designed bilobed flap, which distorts the medial eyelid 4, 5, 6, 7 (▶ Fig. 9.11, ▶ Fig. 9.12, ▶ Fig. 9.13).
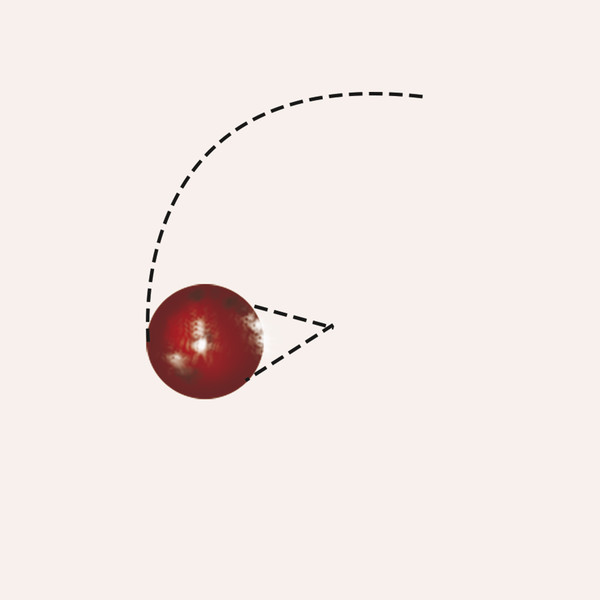
Fig. 9.11 Transposition flap differs from a rotation flap in that the flap tissue is transposed over intervening tissue and into the defect. This allows the transfer of tissue from a relatively tissue lax region to a region of tissue deficit.

Fig. 9.12 The first lobe is designed identical in size to the defect. The dog-ear is excised and the flap elevated in the deep subcutaneous plane. The second lobe is closed primarily prior to inset of the flap.
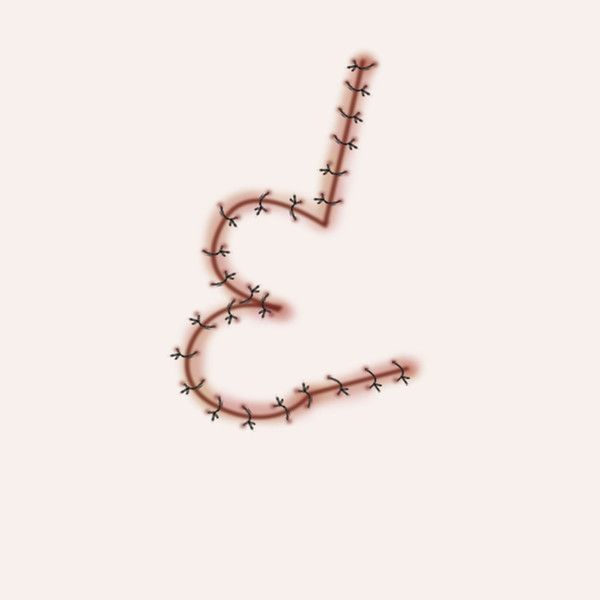
Fig. 9.13 Flap inset.
9.6 Bilobed Flap
The bilobed flap, classic transposition flap, was originally described by Esser in 1918 for nasal reconstruction and made more workable by Zitelli, who limited the arc of rotation to 45 degrees of each limb versus 180 degrees in the original design. 6, 8, 9 Like most transposition flaps, the bilobed flap allows the ability to recruit tissue from a distant site and thus recruit from an area of relative tissue laxity to an area of relative tissue scarcity, which makes it theoretically ideal for transition of tissue from the more lax upper two-thirds of the nose to the less mobile lower third of the nose.
There are, however, significant disadvantages to bilobed flap reconstruction, including complex incision lines that are, by definition, impossible to be placed within relaxed skin tension lines. 9 There is no opportunity to follow principles of subunit nasal reconstruction and an inadequate flap design or execution can result in irreversible nasal deformities of both contour and symmetry. For these reasons, even within the best hands, a bilobed flap reconstruction is never a “perfect” reconstruction, but may well be the most appropriate given the defect.
Modern bilobed flap design is based on the Zitelli modification that limits the arc of rotation of each limb. 8 The first lobe is always designed exactly the same size as the defect and is rotated in position in a relaxed easy fit. The arc of rotation can either be geometrically drawn or free drawn and is a fixed constant based on the diameter of the defect. The donor site of the second lobe actually determines whether the flap design will be successful. Understand that the second lobe is not made 50% of the first lobe size, but is essentially made as large as can be closed without distortion of the second lobe donor site. 6, 8, 10 This determines the suitability of the flap, that is, if the closure of the second lobe is going to result in medial lower eyelid distortion to recruit tissue on the nasal sidewall, the flap design is unsuitable for this location. Zitelli also described a planned dog-ear excision or a standing cone excision on the first lobe that is excised prior to flap elevation. 6, 8, 10
Dermatologist Joel Cook has made multiple observations and provisions for successful flap design, including the preference for a submuscular flap dissection; however, this decision can mostly be left to surgeon preference, as a submuscular dissection provides only a theoretical decrease in pincushioning and is significantly more involved in flap elevation and inset. 9, 10
Principals of successful bilobed flap reconstruction include the initial marking of the arc of rotation for the entire flap and then very careful anatomic measurement of the initial lobe size, which is transposed along the previously drawn arc of rotation. The planned dog-ear excision is outlined and then excised prior to the remainder of the flap elevation. Then, decisions are made regarding the second lobe, which is designed as large as possible to permit primary closure. The second lobe is elevated and the defect is closed with the remaining lobe rotated into position on the inset and then tacking sutures can be utilized even along the pedicle of the flap to improve in particular alar contour. Initial flap sutures are removed at 5 days and dermabrasion offered at 5 weeks. Unfortunately, pincushioning is not an infrequent complication of this flap and is initially managed with sequential low-dose (10%) triamcinolone. If the pincushioning does not resolved after a reasonable period of intralesional management, flap re-elevation, thinning, and re-inset are indicated (▶ Fig. 9.14, ▶ Fig. 9.15, ▶ Fig. 9.16, ▶ Fig. 9.17, ▶ Fig. 9.18, ▶ Fig. 9.19, ▶ Fig. 9.20, ▶ Fig. 9.21, ▶ Fig. 9.22, ▶ Fig. 9.23, ▶ Fig. 9.24, ▶ Fig. 9.25, ▶ Fig. 9.26, ▶ Fig. 9.27).
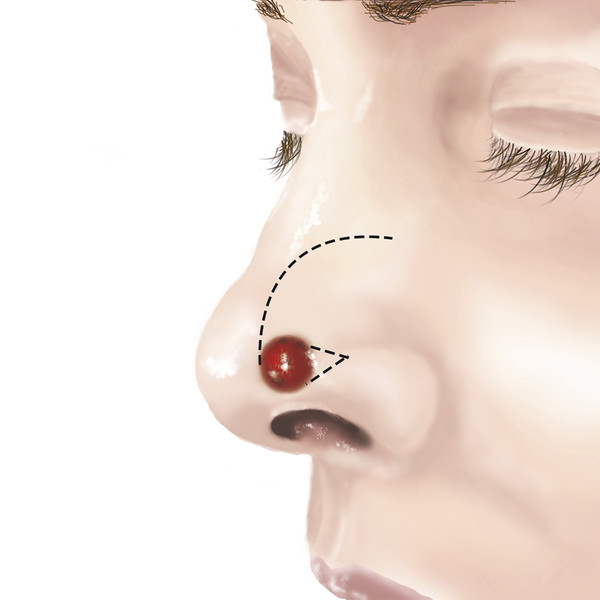
Fig. 9.14 The arc of rotation for both lobes is drawn as well as the planned standing cone excision.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


