Introduction
Over the years, numerous local flaps have been utilized for closure of facial defects. Owing to the robust blood supply of the facial soft tissues, many local flaps have been based on the dermal and subdermal capillary circulation and simply represent the geometric repositioning of the skin and soft tissues. Other flaps, such as the paramedian forehead flap and the nasolabial flap, are based on known vascular systems of the face and have evolved through improved understanding of these systems, as well as refinements in flap design that optimize vascularity. The facial artery musculomucosal (FAMM) and submental flaps are direct descendants of this recent renaissance in our understanding of the vascular systems of the face.
Forehead Flap
Introduction
The forehead flap is one of the first flaps used and reported in surgery of the face. While its origins are unclear, the flap was likely used before the birth of Christ. First known as the median forehead or Indian flap, it has been performed in India since 1440, and the first English descriptions of the flap first appeared in the Madras Gazette in 1793, and a year later in the Gentleman’s Magazine of London . Two cases of nasal reconstruction using the Indian forehead flap were reported in 1816, by the English surgeon, Carpue. In the United States, Kazanjian first promoted the median forehead flap, the design of which included both supratrochlear arteries. Millard demonstrated that the mid-forehead flap could survive on just one supratrochlear artery, which greatly facilitated its transfer to the nasal site. Subsequent refinements in the design and execution of the paramedian forehead flap were described by Burget and Menick. The paramedian forehead flap has evolved as the primary flap for reconstruction of the external cover of the nose due to its texture and near perfect color match to nasal skin. Its robust vascularity, ability to accommodate a wide variety of flap designs, and a very forgiving donor defect make the forehead flap a major workhorse in nasal reconstruction primarily, and for the reconstruction of a variety of adjacent periorbital and cheek defects.
Flap Anatomy ( Fig. 31.2 and Fig 10.1 , Fig 10.4 , Fig 10.5 )
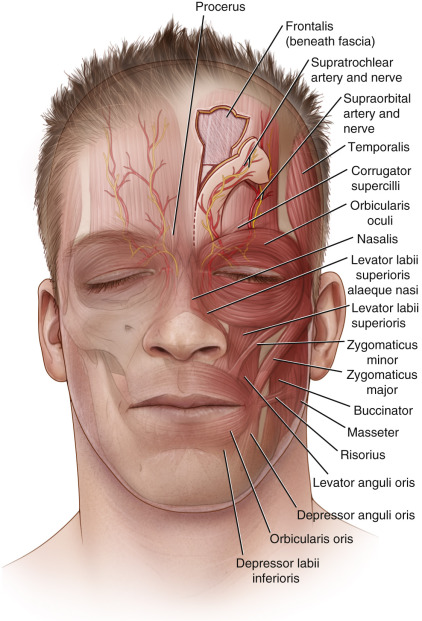
The forehead flap is a versatile flap for reconstruction of the nose and the nasal glabellar region ( Fig. 31.2 ). It is reliable, well-perfused, easily harvested, and has an acceptable donor site. The forehead flap is composed of the skin and subcutaneous tissues of the forehead, including the subcutaneous fat, variable portions of the frontalis, corrugator, and procerus muscles, and a thin fascia/fibroareolar layer contiguous with the scalp galea that lies directly deep to the muscle layer. An interconnecting arcade of the supraorbital, supratrochlear, infratrochlear, superficial temporal, dorsal nasal, and angular vessels provide a rich and versatile vascular supply to the forehead (see Figs 10.4 and 10.5 ). These vessels course superficial to the muscle layer in the subcutaneous fat. The robust vascularity of this region provides for a variety of forehead flap designs. The ancient Indian method of nasal reconstruction utilized a central or median forehead flap based on the vascular plexus created by these vessels. While still utilized, the median forehead flap design limits pedicle length and has a less reliable vascular circulation as it lacks an axial vessel. The paramedian forehead flap is an axial flap that incorporates a vertical arterial branch of the supratrochlear artery and is the most reliable method of transferring forehead tissue for nasal reconstruction.
Arterial and Venous Supply of the Flap
Arterial Supply ( Figs 10.4 and 10.5 )
Dominant:
supratrochlear artery
Length: variable 2–4 cm
Diameter: 0.2–1.5 mm
The blood supply to the paramedian forehead flap is primarily via the axial supratrochlear artery. After exiting its foramen (see Fig. 10.1 ) the supratrochlear vessel courses over the periosteum at the supraorbital rim for a short distance (1 cm) and then divides into deep and superficial branches. The deep branch terminates in several small branches that extend 2–3 cm over the periosteum. The superficial branch continues in a cephalad direction, pierces the frontalis muscle and courses in the subcutaneous fat plane, where it terminates in multiple small branches that anastomose with the subdermal plexus of the mid- and superior forehead.
Other contributing arteries include the dorsal nasal artery, an extension of the angular artery, and the supraorbital artery. These vessels form a plexus that intercommunicates in the superficial periosteal plane at the level of the orbital rim and nasal glabella. Axial extensions of this plexus perforate the frontalis muscle and course in the subcutaneous fat joining a rich subdermal plexus in the upper forehead and scalp. It has been shown that optimal incorporation of the vessels supplying the paramedian forehead flap should include elevation of the periosteum 2–3 cm cephalad to the base of the flap, and preserving 7 mm of tissue above the supraorbital rim as a zone of safety to optimize inclusion of branches from the supraorbital plexus. Experience has shown that these landmarks of elevation can be exceeded if additional flap length is required. As the flap dissection proceeds proximally, however, and the periosteal layer is elevated with a narrowed overlying skin pedicle, the communicating branches from the supraorbital and angular systems may be divided, thereby stifling any benefit of improved perfusion provided by the superior orbital plexus.
Venous Drainage (See Figs 10.4 and 10.5B )
Venous drainage of the forehead flap parallels its arterial inflow with communications between the random dermal plexus of the upper forehead, to the axial supratrochlear system with anastomotic connections to the periorbital plexus, as described above, and the angular system.
Flap Innervation ( Figs 31.2 , 10.11 )
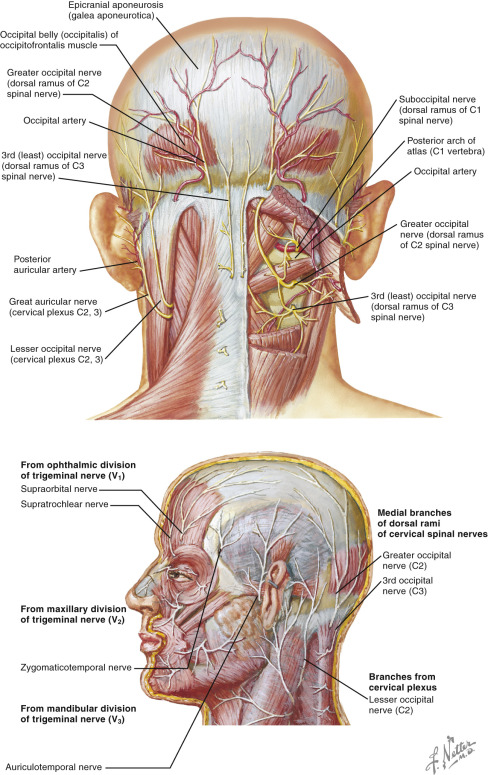
Sensibility in the central forehead is provided via the supratrochlear and supraorbital nerves. Branches of these nerves may be included in the paramedian forehead flap during its elevation, allowing for some cutaneous sensibility. Proximal flaps that are directly transferred and inset around the nasal glabella, dorsum, or sidewall regions may retain their sensibility. The more common distally targeted flaps, based on a supratrochlear pedicle, lose sensibility following pedicle division.
Flap Design
Anatomic Landmarks ( Case 31.1 , Fig. 31.3 )
Design of the forehead flap is based on a template of the defect that is centered over the supratrochlear artery. Using a handheld Doppler, the course of the supratrochlear artery is identified and marked from its origin from the supratrochlear foramen on the medial orbital rim to the mid-forehead. A foil template of the defect is made. Foil derived from suture packet is ideal for this purpose, as it has a shiny side and a color side that can be helpful in demarcating the “skin” and “subcutaneous” sides of the flap – a simple way to ensure the accuracy of flap design and minimize the potential for inadvertent reversal of the pattern and the harvest of a backward flap. An ipsilateral paramedian forehead flap permits the maximum arc of rotation. A left-sided flap should rotate counter clockwise, and a right-sided flap, clockwise. This orientation will provide the shortest distance between the flap pivot point and the nasal defect and place the skin of the forehead flap facing the ipsilateral eye, as opposed to the raw surface underlying the flap, which is preferable in terms of patient comfort. The arc of rotation of the flap should be carefully measured from the vascular base of the flap, which serves as the pivot point. This should be placed at the nasal root of the medial brow. Palpation of the bony landmarks of the orbit can facilitate the location of the proper pivot point. The flap pivot point can be extended inferiorly to gain further reach if periosteal release and meticulous dissection of the vascular pedicle are carried out in the subperiosteal plane. This should be performed under loupe dissection for proper identification and preservation of the supratrochlear vessels. It is important to accurately assess the true flap pedicle length. An overly tight inset can compromise the vascularity of the distal forehead flap or compromise the integrity of the reconstruction by elevation or distortion of the underlying framework and lining. Redundancy of the flap pedicle may be troublesome to the patient in terms of interference with the nasal visual field.
Because of the position or size of the forehead flap in relation to the frontal hairline, hair-bearing scalp tissue may need to be included as part of the flap. This issue must be carefully addressed and discussed preoperatively and particularly with those patients having a relatively short forehead, and/or those having a distal nasal defect such as one involving the columella. The hair can be depilated during flap harvest in a non-smoking patient by thinning the distal 1–1.5 cm of the flap, or it can be removed at a later juncture. If there is any doubt as to the integrity of the flap’s vascular supply, it is best to delay thinning/depilation for a subsequent revision.
An alternative to extending the flap into the frontal hairline has been proposed by Reece et al. This modified version of the paramedian forehead flap incorporates the vertical axis of the supratrochlear system and an oblique, hairless forehead extension that is based on the subdermal plexus supplied via the terminal branches of the supratrochlear system. This flap also includes perforators from the deep periosteal branch of the supratrochlear artery, and the three-vessel flow supported through the superior orbital plexus.
The paramedian forehead flap should be designed with a base of 1.2–1.5 cm in width at the pivot point directly overlying the supratrochlear vessels. A wider flap base is at risk for compressing the feeding vessels when the flap is rotated.
In nasal reconstruction, a lining component of the forehead flap can be included in the design for the external cover. The flap template can be extended to include portions of the vestibular lining and/or columella. This technique has utility provided that the lining defect is not excessive. In these situations, the dimensions of the missing lining are added as a distal extension to the alar margin of the external cover template. The lining extension is made larger than needed to accommodate a relaxed folding – about 4–5 mm during inset to avoid compromising the dermal perfusion of the distal flap elements. Utilizing this approach, the flap is folded on itself and inset. Flap debulking and placement of cartilage grafts to achieve the desired contour and dimensions of the reconstruction are performed in a secondary procedure.
General Thoughts About Flap Design
The paramedian forehead flap is quite reliable with a robust vascular supply. The key to success with the flap is axial orientation of the long axis of the flap template directly overlying the course of the superficial branch of the supratrochlear artery. In isolated patients the supratrochlear system may be very small or undetectable via Doppler. In these cases the opposite side should be examined, and if the supratrochlear system is identified, the flap should be based on this side. If neither side exhibits an identifiable supratrochlear artery, delay of the template over the anticipated course of the supratrochlear system may be required. Following flap design, an incision is made around the flap perimeter to just above the periosteal layer and then closed with fine sutures. In 14–21 days the flap is elevated and examined for adequacy of perfusion. If mottling or hypoperfusion is identified, further delay is warranted.
Flaps based on the supratrochlear system may have a variety of configurations and sizes depending on the reconstructive requirements. As demonstrated by Reece et al., random dermal extensions beyond the linear axial course of the supratrochlear artery can be included to avoid the hair-bearing scalp.
Flap Dimensions
Flaps measuring 8–9 cm in width and encompassing the length of the forehead can usually be elevated primarily without delay. Additionally, random extensions oriented obliquely beyond the axial line of the supratrochlear system can be safely included in flap design. Extensions of the flap superiorly into the frontal hairline beyond 1–1.5 cm are unpredictable with regards to reliability and should be delayed.
Technique of Flap Harvest ( Case 31.1 , Fig. 31.3 )
Primary elevation of the flap is performed incorporating the skin, subcutaneous, frontalis muscle layer, and the submuscular fibroareolar layers of the forehead. Dissection is begun from the superior forehead to the base of the pedicle. Following incision of the flap perimeter, dissection is carefully performed just above the periosteal layer. It is important to not elevate the periosteal layer of the superior forehead to avoid frontal bone exposure and delayed healing, and epithelialization of the donor defect. As the dissection proceeds to within 2–3 cm from the base of the flap, the periosteum is included with the flap base to include the periosteal branch of the supratrochlear artery. Flap perfusion is further optimized by limiting the skin incision to 7 mm above the supraorbital rim so as to optimize inclusion of vascular contributions from the supraorbital plexus.
The distal 15 mm of the flap can be thinned of its muscular and subcutaneous layers in the primary setting provided that the longitudinal subcutaneous veins, coursing in the superficial subcutaneous layer just below the dermis, are preserved. This facilitates flap insetting in the tip, columella and alar rim. For folded forehead flaps, thinning is delayed until the second procedure in which the lining element is separated from the external cover. At this time, the lining can be aggressively thinned to its dermis.
The flap is inset in layers with fine monofilament absorbable sutures for the deep muscular layer and percutaneous polypropylene sutures for the skin. Where the flap has been thinned prior to inset, a simple percutaneous suture closure is employed. If excessive tension is encountered during inset of the flap, this can be partially relieved by insetting the muscle layer of the forehead flap to the skin or mucosal layer of the target defect. The resulting subcutaneous “gap” at the site of inset will eventually heal by secondary intent with local wound management to prevent drying. In these cases, liberal amounts of ointment are applied to the open wound areas during healing.
After the flap is inset into its target defect, the undersurface of the flap pedicle is temporarily closed with a split-thickness skin graft. This approach is favored over wound dressings as the skin graft will “take” to the undersurface of the flap pedicle, stifling the messy blood and serum ooze that occurs postoperatively. The skin graft is placed without tension and trimmed to match the defect. It is inset with 5-0 chromic catgut suture.
Donor Site Closure and Management
Closure of the donor defect may be primary, with a skin graft, or by allowing healing via secondary intent. Each method has certain advantages. Primary closure of the donor defect is generally reserved for smaller flaps <2.5 cm in width. Minimal submuscular undermining is required to close with minimal tension. Skin graft closure is preferred for flaps that are excessively wide, especially at the base, where primary closure will distort the position of the medial brows resulting in an unaesthetic, unnatural facial/periorbital appearance. The graft is usually removed and replaced by re-insetting the proximal flap pedicle into its original defect following forehead flap division and inset.
Flaps having a narrow (1.5 cm) base but with a wider superior distal defect on the forehead, can be managed by primary closure of the proximal defect and allowing the superior or distal defect in the mid- and upper forehead to heal by secondary intent. In this sitting, wide submuscular undermining of the forehead is performed to gain sufficient mobilization for closure of the lower 4–5 cm of forehead with minimal tension. This also provides for partial closure of the mid- and upper forehead defect minimizing the size of the remaining wound that will eventually heal by secondary intent. It is important to not allow the exposed periosteum to dry, as this will result in necrosis of the periosteum and eventual exposure of the frontal bone, leading to delayed healing and possibly the need for additional surgical intervention. We have found it helpful to cover the exposed periosteum with petrolatum-impregnated gauze until epithelization commences and a granulation base is established. At this point, the wound is managed with topical Preparation H or A&D ointment and a Telfa pad until epithelization is complete. Moisturizers are then applied thereafter. Avoid topical antimicrobials containing silver as the silver may leach within the substrate of the migrating epithelium leading to undesirable pigmentation of the wound.
Drains are generally not required for the forehead undermining and closure. A benefit of allowing the forehead donor site to heal by secondary intent is complementary pigmentation of the epithelized defect with excellent color match to the surrounding forehead skin. Following flap division, the proximal pedicle stump is re-inset into the base of the donor defect as an inverted “V.”
For forehead donor sites that result in unacceptable scarring, the adjacent normal forehead skin may be expanded to replace the scar. Alternatively, epidermal overgrafting of the scar can be performed using split scalp grafts resulting in substantial improvement in color.
Flap Usage
The forehead flap is indicated for all varieties of nasal external cover and limited nasal vestibular defects ranging from isolated alar or tip defects to total and subtotal nasal external cover defects. In rare situations, two forehead flaps may be utilized to provide for both lining and external cover. Large lining defects involving the vestibule and middle nasal vault are best managed with remote free flaps such as the radial forearm flap, reserving use of the forehead flap for external cover.
The forehead flap may also be utilized for a variety of periorbital defects resulting from cancer ablation or trauma. The design of the flap can be quite elaborate as long as its major axis is centered over the course of the supratrochlear artery. Flap design in this setting is critical to ensure that the important distal part of the flap reaches its intended target without tension or kinking of the pedicle. Designing the flap template 2–3 mm larger than the defect provides for a margin of safety to ensure sufficient dimensions for closure without tension.
Postoperative Care and Expected Outcomes
In most cases the forehead flap is transplanted to its target defect as a pedicled flap. As noted above, in these instances the undersurface of the pedicle is closed with a split-thickness skin graft to facilitate wound management. The skin graft suture line is dressed with a light application of antibiotic ointment. The inset portion of the forehead flap is similarly left open and dressed with a light application of antibiotic ointment, applied twice daily following suture line cleansing. Skin sutures are removed at 5–6 days and the wound is then reinforced with fine skin tapes for, an additional week.
The robust blood supply of the forehead flap allows for excellent healing in most circumstances. In smokers, in patients with systemic vascular disease, or in patients having scarred foreheads in which the axial or random aspects of the forehead blood supply have been damaged, flap ischemia and necrosis can complicate the anticipated outcome. In these settings it is prudent to anticipate problems beforehand so as to minimize the morbidity of delayed healing and flap failure. If a Doppler signal cannot be detected prior to flap elevation, if the flap appears mottled following elevation, or has areas that appear to be poorly perfused, it may be best to delay the flap. As well, if scar traverses a portion of the flap, and there are no reasonable alternatives for flap location, it is best to consider delaying the flap to optimize its perfusion.
FAMM Flap
Introduction
The facial artery musculomucosal flap (FAMM) is an axial flap based on the facial artery that is very useful for coverage of soft tissue defects of the oropharynx and nasopharynx, as well as the lip. First described by Pribaz et al. in 1992 as an evolution of the buccal mucosal flap, reports of the FAMM flap have been widely reported in the literature. Indications are not limited to oncologic and traumatic reconstruction, as the FAMM flap is especially useful in the management of refractory palatal fistulae following treatment for cleft palate. The flap is harvested as a pedicled flap and may not be used as a free flap, given that venous drainage relies on a robust venous plexus rather than a discrete, named vein. It may be superiorly or inferiorly based, which gives it significant versatility and arc of rotation that allows its application for a wide variety of defects.
Flap Anatomy (See Fig 10.4 , Fig 10.5 )
The FAMM flap is harvested intraorally and is based on the facial artery. As the facial artery courses across the cheek, it lies superficial to the buccinator muscle, which is the deepest muscle of the sphincteric system of the mouth. Deep to the buccinator muscle lies the submucosa and oral mucosa. Near the oral commissure, the facial artery is also deep to the lateral edge of the deep lamina of the orbicularis oris muscle as well as the levator anguli oris muscle, and may be superficial or deep to the levator labii superioris muscle.
When harvesting the FAMM flap, it is important to consider the course of the parotid duct. The parotid duct exits the parotid gland and courses through the buccal fat pad before piercing the buccinator muscle and entering the mouth at the level of the second maxillary molar at the parotid papilla.
Arterial and Venous Supply of the Flap (See Figs 10.4 and 10.5 )
Arterial Supply of the Flap
Arterial supply of the FAMM flap is based on the facial artery. After crossing over the inferior border of the mandible at a mean of 6.5 cm from the symphysis, the facial artery gives off small muscular branches to the masseter and the depressor anguli oris muscles. The facial artery then follows a tortuous course obliquely upward and gives off the inferior labial artery at the inferior border of the buccinator muscle along with the sublabial artery (labiomental artery), approximately 70% of the time. The facial artery ultimately comes to a point 1–2 cm lateral to the oral commissure, where it gives off the superior labial artery as well as 3–5 branches to the buccinator muscle and a small superficial branch to the zygomaticus major muscle. From this point, the anatomy of the facial artery is highly variable. Approximately 80–90% of the time, the facial artery continues as the lateral nasal artery and gives off both superior and inferior alar arteries before either terminating as the superior alar artery or continuing as the angular artery before terminating near the medial canthus. The remainder of the time, the course of the facial artery may include a separate takeoff of the angular artery after crossing the inferior border of the mandible, septal and inferior/superior angular arteries branching from the superior labial artery, or a rudimentary facial artery that gives off inferior labial artery only. Even within individuals, there is variation between right and left sides of the face as the facial artery branching and termination pattern is only considered to be symmetric approximately 50% of the time.
Dominant:
facial artery
Length: 7–8 cm
Diameter: 1.7 mm (1–2 mm)
After crossing over the mandibular border, the diameter of the facial artery is 2.6 mm (range 1.6–3.6 mm). It decreases to approximately 1.7 mm over its course as it nears the oral commissure.
Venous Drainage of the Flap (See Figs 10.4 and 10.5B )
Primary:
subdermal plexus
Venous drainage of the flap is provided by a robust venous plexus that envelops the facial artery along its course and communicates with the pterygoid plexus and internal maxillary vein posteriorly, and the facial vein anteriorly; no discrete named vein is included in the flap.
Flap Innervation
There are no sensory or motor nerves that are harvested with the FAMM flap.
Flap Design
Anatomic Landmarks ( Case 31.2 , Fig. 31.4 )
First, the course of the facial artery is identified by Doppler along the buccal mucosa surface intraorally, and is marked along its course from the retromolar trigone to the gingivobuccal sulcus. The entire length of the facial artery as it traverses the buccal mucosa can be included in the flap if necessary. The width of the flap is next determined, and can include up to 3 cm of buccal mucosa as needed for the reconstruction. Special care should be taken to avoid injuring Stensen’s duct, which enters the mouth adjacent to the second maxillary molar. Flap design should remain anterior to the duct.
General Thoughts About Flap Design
The FAMM flap is an axial flap and must follow the course of the facial artery. The facial artery courses obliquely through the cheek; therefore, the flap design should be obliquely oriented as well.
The connection between the facial artery and the buccinator muscle contains small communicating vessels that provide nourishment to the overlying buccal mucosa. This connection between the buccinator muscle and the facial artery is somewhat tenuous, and care must be taken to ensure that the artery and muscle do not become separated during flap elevation and inset.
Although venous drainage from the FAMM flap via a robust venous plexus envelope the facial artery, this plexus arrangement is fairly efficient. The base of the flap should be kept wide and the facial artery should not be skeletonized as this may interrupt the venous outflow.
A maximal flap mucosal width of 3 cm may be used; however, closure of these wider flap donor site defects may lead to tethering of the cheek and restricted jaw movement. If it is felt that the buccal mucosal closure is excessively tight, a full-thickness skin graft may be utilized to close the defect. Alternatively, triangular mucosal V-Y advancement flaps may be utilized to ease tension on the closure. These adjunctive procedures may be performed at a later stage as well.
Flap Designs for Particular Types of Reconstructions
The FAMM flap is either superiorly or inferiorly based. In all cases, the flap is elevated and transposed into the target defect. If the target defect is in continuity with the flap donor site, direct transfer and inset is performed. If the flap must traverse intact oral mucosa to reach its target defect, the flap’s distal end is inset and the pedicle is divided in a second stage 10–14 days later. This is particularly useful when treating defects of the palate or floor of mouth that are lingual to the alveolus. In these cases, a bite block should be used to protect the pedicle when teeth are present. However, it is possible to route the flap posteriorly in the retromolar region to treat certain palatal or floor of mouth defects, allowing inset of the flap in one stage without the need for secondary division. When routing posteriorly, the mucosa posterior to the molars may be divided, excised, or elevated and used for other purposes.
The FAMM flap can be used for reconstruction of the nasal lining provided that the defect is at the level of the middle nasal vault or posterior to this. Anteriorly placed FAMM flaps in the nasal vestibule may produce excessive mucus that can be an annoyance with constant nasal discharge and crusting. If used for nasal lining, the FAMM flap is superiorly based. Access to the nose is gained through a gingivobuccal sulcus incision, and the flap is tunneled through the piriform aperture into the nasal vault. When closing this incision, the mucosa of the flap should be gently separated from the buccinator muscle attachments during its course from the intraoral to the intranasal space allowing for direct mucosa to mucosa closure of both spaces, thus circumventing the development of an oronasal fistula.
The FAMM flap has great applicability for lip and vermillion reconstruction. Orientation of the facial artery pedicle lends itself well to transposition of these flaps with primary inset. So as to avoid donor site morbidity, the design and elevation of long thin flaps is desirable. Compared with tongue and cross-lip flaps that require secondary division and inset, the FAMM flap carries a significant advantage in being completed in one stage. Additional advantages of the FAMM flap for lip and vermillion reconstruction include its bulkiness and complementary color match.
Flap Dimensions
Width: 1–2 cm, maximum 3 cm
Length: 5 cm, maximum 7–8 cm
Technique of Flap Harvest ( Case 31.2 , Fig. 31.4 )
The patient is placed in the supine position with the neck slightly extended and a shoulder roll used if necessary. A Dingman mouth prop, bite block, or dental molt may be placed in the mouth in order to facilitate exposure. Alternatively, retraction sutures may be used instead to facilitate exposure and dissection. Next, the course of the facial artery is determined by Doppler exam and is then marked on the oral mucosa. The flap width is determined by the size of the defect, and the flap is then designed to be centered on the facial artery. An incision is then made across the distal end of the flap (either superior or inferior depending on the flap orientation), and dissection is carried through the mucosa, submucosa, and buccinator muscle, until the facial artery is identified and ligated. Incisions paralleling the facial artery are then made on the anterior and posterior sides of the flap, and dissection is again extended through the buccinator muscle with direct identification of the facial artery. The flap is then elevated from distal to proximal, taking special care to include the facial artery within the flap. Once the flap is elevated in its entirety, it is transposed into the defect. It is important to preserve a cuff of soft tissue/adventitia around the facial artery during flap elevation to avoid injury to the venous plexus and hence, venous drainage from the flap.
Donor Site Closure and Management
A two-layer closure of the donor site is typically performed using 4-0 synthetic absorbable polyglactin or polydioxanone suture to approximate the buccinator muscle and 4-0 chromic catgut suture to close the buccal mucosa. Postoperatively, the patient is placed on a puree diet for 3 weeks and prescribed an antibacterial mouth rinse to be used post-prandial and at bedtime.
Flap Usage
Indications: The FAMM flap is used for reconstructions of the oropharynx, including the lips and vermillion, and the nasopharynx.
When the flap is superiorly based, the arc of rotation allows it to treat defects of the palate, upper gingivobuccal sulcus, nasal lining, upper lip, and the orbit. When the flap is inferiorly based, it may be used to close defects of the floor of mouth, tonsillar region, alveolus, lower lip, and mandibular gingivobuccal sulcus.
Postoperative Care and Expected Outcomes
In general, patients who have undergone FAMM flaps do not require specialized care. They may begin a liquid diet on the day of surgery, and progress to a puree diet starting on day 3. By 3 weeks, the patient can return to a regular diet. When performing a lingually placed FAMM flap in a patient with intact dentition, a bite block should be secured in place to protect the pedicle until after pedicle division and inset.
Owing to the proximity of the facial artery to the levator anguli oris, the levator labii superioris and the orbicularis oris muscles (see Figs 10.1 , 10.5 ), some weakness in animation of the lips may result from flap harvest. While careful elevation of the flap from its bed will minimize injury to these muscles and their respective motor nerves, it is important to discuss these risks with the patient beforehand.
As noted above, the donor defect resulting from harvest of a wide flap (2.5–3.0 cm) will necessitate closure under tension if closed primarily. This may result in restriction of jaw opening, dysfunction of the buccinators, and possible obstruction of the parotid duct flow. In these cases, the application of a full-thickness skin graft or use of local mucosal flaps to decrease tension on the donor site closure may be required.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


