Summary
The most frequently indicated revision for local flaps is correction of contour abnormalities. The final result is best if maximal scar maturation is achieved prior to revision.
Alar contour abnormalities often require direct alar rim incision and significant soft-tissue debulking along nasal sidewall.
Incisions across the very vascular face can be made with little regard to previous incisions.
24.1 Complications and Their Management
24.1.1 Noninvasive Management
The issues with local flaps involve early healing with contour abnormalities, as well as color. Most color issues including poor border scar appearance can be addressed with judicious scar management like any other Mohs procedure. This includes early (6 weeks) dermabrasion and pulsed-dye laser if indicated for color. 1, 2 The management of contour abnormalities, particularly with interpolated bilobed flaps or posterior labial flaps, entails early scar care with massage, which has proven to be remarkably efficacious, as well as a light dose of steroid injection. 2, 3, 4 Understand that straight volume requirement or disruptions of natural creases are rarely improved to the point of not requiring later revision surgery and the role of scar massage and Kenalog should be viewed as optimizing the appearance prior to definitive surgery. For this reason, the use of multiple rounds of laser therapy might best be saved until after the final revision when the contour is right to improve the final color for the patient’s lifetime result (▶ Fig. 24.1, ▶ Fig. 24.2, ▶ Fig. 24.3).
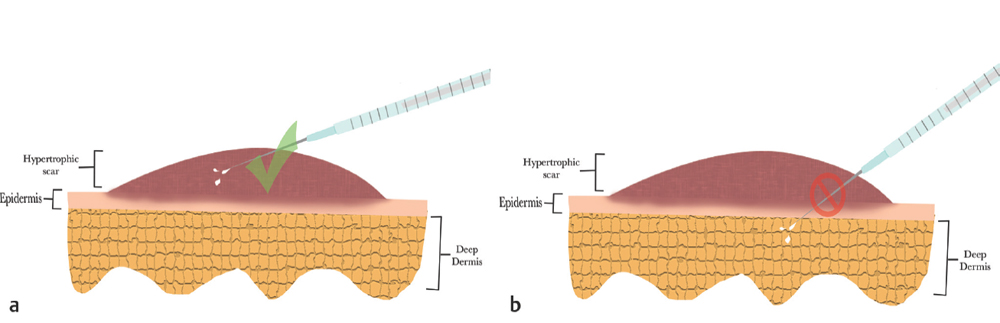
Fig. 24.1 (a) It is extremely easy to inject underneath lesion, which will only lead to long-term and often irreversible fat atrophy. (b) To avoid this, the scar tissue itself must be injected with a Luer Lock needle and syringe.

Fig. 24.2 A 53-year-old female status post ergotrid flap that resulted in pincushioning. Pincushioning resolved over time with appropriate scar care, including silicone sheeting, scar creams, and three cycles of 20 mg/mL of 2- to 10-mL Kenalog injection over 18 weeks. Final results shown after 1 year.

Fig. 24.3 (a) A 59-year-old female status post direct closure of Mohs defect at left cheek. Patient shown at 5 days and 2 weeks postoperatively prior to scar management. Patient expressed concern over scar redness. Laser treatment initiated 1 month postoperatively. (b) Results shown 1 month after first laser treatment with 532-nm wavelength at 6 J for 3 ms at 7-mm spot size and 2 weeks after second laser treatment with 532-nm wavelength at 6.2 J for 3 ms at 7-mm spot size. (c) Final results 5 months postoperative shown 1 month after third laser treatment with 532-nm wavelength at 6.2 J for 3 ms at 7-mm spot size completed.
24.1.2 Revision Surgery
When the decision to proceed with revision surgery is made, very careful assessment of the patient’s perception of the defect is paramount to ensure that it matches the surgeon’s. Other factors important to consider in this decision making are the multiple variables that contribute to final scar appearance, including the patient’s persistence, the wound healing phase or the stage of wound healing, and the severity of the defect. Understand that left entirely with no other factors and left entirely to the plastic surgeon, the majority of plastic surgeons would elect to perform scar revisions somewhere in between 18 to 24 months when maximal healing is allowed. 2 However, when there is an untoward scar on somebody’s face, now is not the time to either be dogmatic or academic and it is best to weigh all the factors regarding management of revisions. If one is able to achieve a reasonable facial result with an early initial revision, then “time is on the surgeon’s side” and one is able to wait a great deal longer prior to planning of the next or often final stage of surgery. Simple flap contour deformities will worsen the border scar appearance just from the shadowing and highlighting and the would-be flap is able to be re-elevated. A significant amount of thinning can be performed safely even to the point of re-elevating the flap 100% and base the circulation on the deep soft tissue, and one is able to provide an improvement in contour across the entire border (▶ Fig. 24.4, ▶ Fig. 24.5, ▶ Fig. 24.6, ▶ Fig. 24.7).

Fig. 24.4 A 65-year-old female status post Estlander flap. This case illustrates why the practice at UTSWMC has abandoned the use of Estlander flaps as it completely obliterates the very difficult-to-reconstruct oral commissure. Revision required re-elevation and re-inset of the flap with simultaneous commissuroplasty. Final postoperative results shown at 9 months.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


