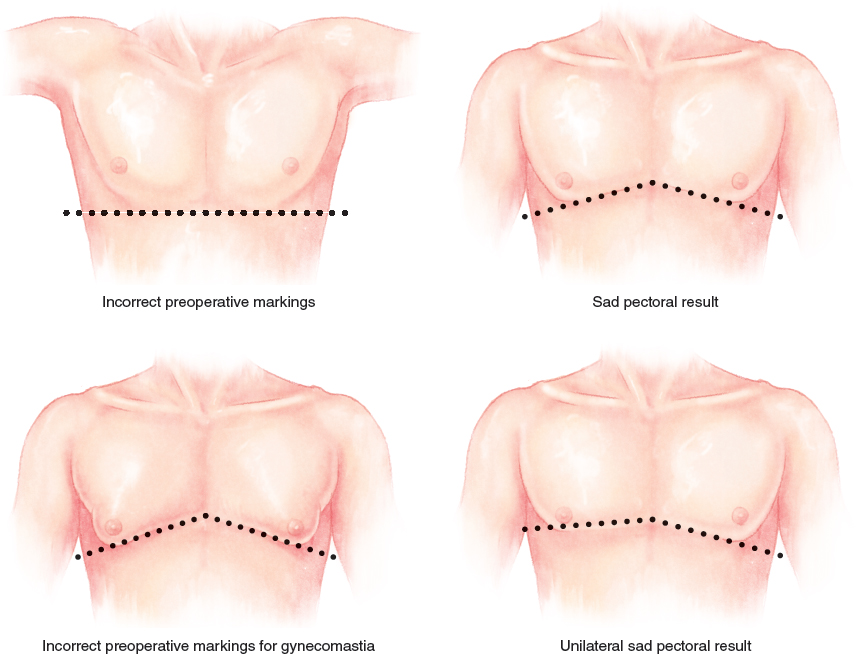
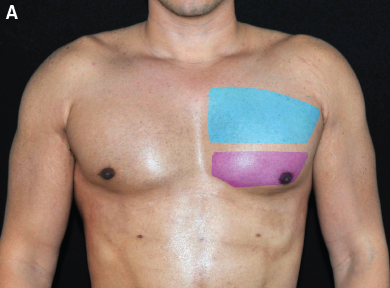
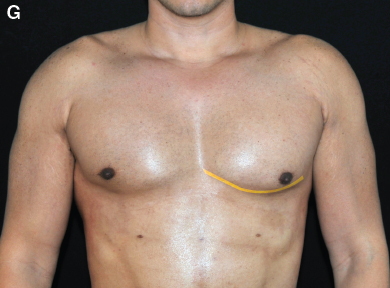
CHAPTER 21 Alfredo E. Hoyos Fig. 21-1, A In men, cosmetic surgery should focus on restructuring the upper torso through selective liposuction and fat grafting to transform the body type into a more athletic appearance. The V-shaped body is only a desirable feature for men. Fig. 21-1, B In women, the features are more feminine and delicate, so reduction of the upper torso results in a younger, slimmer look. Fig. 21-2 The upper torso is divided according to the muscles that have key influence on the shape of the area. With this concept, certain muscles are considered “alpha” muscles. Although an alpha muscle may be the largest one in the region, sometimes it is the impact that a specific muscle has on the silhouette that justifies this designation. In the anterior view, the main muscle is the pectoralis major, which is obviously important because of its size and mass. The other muscles that are involved in the upper torso outline are the muscles of the arm. The alpha muscle of this area is the deltoid. This may seem counterintuitive, because the other two muscles of the upper arm—the biceps and the triceps—are stronger. However, although the deltoid is not the biggest muscle of the arm, it is the one that gives the impression of power and health and that contributes to the V shape of the torso. In this chapter we will demonstrate how to improve the upper torso with the use of liposuction and fat grafting in the chest and arms. The development of the pectoralis muscle is directly related to chest shape and aesthetic standards. Conditions such as abnormal fat disposition, gynecomastia, trauma, and congenital abnormalities distort the normal anatomy and are therefore common motivating factors for requesting reshaping surgery. In addition, correction of poorly developed pectoral muscles is increasingly being requested by men. This poor development is frequently a result of the modern lifestyle in which daily activities do not require much pectoral strength, a high caloric intake, and a lack of physical exercise. Interventions that can be performed on the male chest have been divided into three groups: 1. Pectoral implants for augmentation 2. Fat removal for a fatty or glandular chest 3. Correction of the deformity through the use of flaps, fat transposition, or both Implants have long been the benchmark treatment for pectoral deficiencies. However, implants are expensive, and there are a number of associated complications that can cause unnatural results and a feminized appearance. Many alternative techniques have been described, but none of them achieves the desirable standard. Fat grafting with superficial liposuction sometimes produces better results than those obtained with the traditional methods, so it is a good alternative for male chest reconstruction. The ideal chest appearance is defined by the exposure of the superficial anatomy, which reflects the disposition and development of the pectoralis muscles and the shape and definition of the surrounding tissues. Fig. 21-3, A To fulfill the goals of this technique, the pectoral area is divided into specific zones. The pectoralis muscle is divided into superior (blue) and inferior (purple) poles. The superior pole has a larger volume than the inferior pole because of its greater muscle mass. Five “negative spaces” (green and orange) surround the pectoralis muscle in male patients. These areas should be concave to improve the convex appearance of the pectoral area. Fig. 21-3, C The first negative space is a rhomboid between the inferior borders of the pectoralis major, the xiphoid process, and the origin of the rectus abdominis at the midline. This is known as the interpectoral rhomboid. The second area is a triangle defined by the pectoral line and the lateral border of the rectus abdominis known as the subpectoral triangle. This area links the definition of the pectoralis with the definition of the abdomen. It must be treated aggressively with subdermal and intermediate liposuction. Fig. 21-3, E The third area is the triangular area between the lateral border of the pectoralis muscle and the lateral border of the latissimus dorsi muscle, which is called the pectoralis-latissimus triangle. Although this triangle is beyond the pectoral area, its contouring is important to expand the concavity to this limit. The fourth area, called the subclavicular triangle, is defined as the triangular area between the subclavicular line where it meets the deltoid muscle and the upper border of the pectoralis major. Fig. 21-3, G The fifth area is a curving horizontal line along the inferior border of the pectoralis muscle, usually 1 cm below the nipple level. Known as the pectoralis line, it tilts upward when the muscle contracts to create another line that follows muscular movement. The zone between these two lines is called the dynamic transition zone. This area is treated as a negative space that softens as it goes toward the upper pole. Fig. 21-3, I In male patients, there is a final triangular area (yellow) defined by the inferior lateral border of the pectoralis muscle and by a line that connects the point of the internal border of the pectoralis line with the lateral insertion of the pectoralis muscle. For obese and gynecomastic patients, deep liposuction has to be performed in this area, and this may sometimes extend to the limits of the fat beyond the pectoralis muscle. Fig. 21-5 Throughout the procedure, a pinching maneuver of the pectoralis should be used to locate the position of the tip of the grafting cannula to prevent thoracic puncture. ■ Marking the borders of the pectoralis muscle can be challenging, because different contour deficiencies can be easily reached. If the arms are abducted (up), the anatomic regions will be marked incorrectly. Thus the patient must be marked with the arms in complete adduction. Another critical region is the tissue behind the nipple (mammary disc). A critical margin for resection must be marked to prevent the gynecomastic appearance (sad pectoral) that results from a lack of continuity of the pectoralis major line. ■ In the pectoral inferior triangle previously described (dynamic transition zone), deep liposuction can be freely performed. However, fat should not be extracted from the upper pectoral pole, which is out of the area of this marking. Instead, this area often requires fat grafting. ■ Inadequate marking of the pectoral muscles with the arms in abduction or a lack of accuracy of the markings under the nipple in patients with gynecomastia can produce an inaccurate shape of the pectoralis line (sad pectoral). ■ A cannula with 30 degrees of curvature should always be used for fat grafting. The curvature should always face up to follow the shape of the muscle and to avoid the thoracic cavity. It is of critical importance that the lead surgeon perform this step. Liposculpture with fat grafting is indicated for patients with underdeveloped pectoral muscles, abnormal fat disposition, and gynecomastia. It can also be used for athletic patients who wish to improve the contour and appearance of their pectoral muscles. This is also a good alternative for patients with contraindications for the use of chest implants, such as body builders, who often exercise the pectoralis muscles, and patients with a risk of developing capsular contracture with the placement of implants. Liposculpture with fat grafting should not be performed in patients with major medical conditions such as disorders involving collagen, scarring, or connective tissue; clotting disorders; lupus erythematosus; diabetes; heart disease; lung disease; vascular problems; uncontrolled endocrine disorders; high blood pressure; and psychiatric conditions such as major depression. It should also not be performed on patients receiving anticoagulation therapy. These procedures are relatively contraindicated for massive-weight-loss patients and obese patients who have marked laxity of the skin. These procedures are not designed to be weight-loss techniques. Patients must be instructed that they cannot smoke, use recreational drugs, and drink alcohol excessively for at least 6 months before the procedure. The procedure is performed according to the patient’s body biotype. For this purpose, patients are divided into four groups: slim, athletic, fat, and gynecomastic. Fig. 21-6 In slim patients, definition is created through superficial liposuction. Fat grafting is then performed in the muscular and submuscular layers. Fig. 21-7 In athletic patients, achieving definition requires performing both deep and superficial liposuction. In selected patients, fat grafting can also be used, and some patients will require supramuscular grafting. Supramuscular grafting can be performed in athletic individuals, in whom liposuction does not need to be as extensive and deep. This diminishes the potential for fat migration after tunneling in the supramuscular layer. For fat or pseudogynecomastic patients, liposuction is performed to remove all of the deep fat tissue in and around the pectoralis area. Superficial fat removal plays an important role in achieving skin retraction in this area. Fat grafting is also performed in the superior pole to replace the volume extracted in the inferior pole, thereby providing a lifted appearance.
Liposculpture of the Chest and Arms
 David E. Guarin
David E. Guarin


The Alpha Muscle

CHEST LIPOSCULPTURE
Surgical Anatomy




Indications and Contraindications
Patient Evaluation and Preoperative Planning


Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine