Lipoabdominoplasty is one of the most frequent abdominal body contouring procedures performed today. It guarantees a safe combination of abdominoplasty and liposuction while minimizing the risk of ischemic flap complications. This is because of the limited undermining performed and the liposuction adjunct, both of which minimize perforator injury. In the last several years, the integration of anatomic definition through the use of liposuction has further refined the procedure, led to improved results, and increased patient satisfaction. The more natural results of the anatomic abdominal definition is a next step in abdominal contour refinement.
Key points
- •
Lipoabdominoplasty preserves abdominal wall vascular anatomy through the preservation of the perforating vessels. Dead space is also reduced.
- •
Liposuction-initiated anatomic definition using individualized marking increases abdominal contour and aesthetic results.
- •
Perforator preservation and Scarpa fascia suspension are the fundamental reasons for the decreased morbidity with this technique.
- •
It is a standardized step-by-step technique that is safe and easily reproducible by the practicing plastic surgeon. It will result in optimal aesthetic results when incorporated into one’s practice.
- •
Because patients worldwide are demanding liposuction combined procedures, surgeons should be familiar with this technique.
Introduction
The aesthetic and functional deformities of the abdomen are characterized by skin flaccidity, lipodystrophy, and diastasis of the rectus abdominis muscles.
In the last two decades, lipoabdominoplasty (LAP) has changed the concepts regarding abdominal flap undermining. Limited undermining combined with liposuction has replaced the wide undermining of the traditional abdominoplasty. The result is a preservation of the important abdominal perforators of the deep inferior epigastric artery and a significant reduction in ischemic flap problems postoperatively. In addition the patient notes a better aesthetic result and improvement in body contour.
Although the technique is reproducible and aesthetically satisfactory for most patients when performed step by step according to our described technique, one adverse sequelae is an overly flat lower abdomen.
The anatomic abdominal muscular definition, or high-definition, abdominoplasty came about through retrospective review of our earlier surgical results. Midline definition has ushered in yet a newer phase of abdominal contouring.
Principles of lipoabdominoplasty with definition
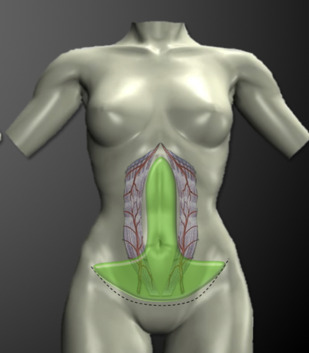
The fundamental principle of this technique is still the preservation of abdominal wall perforators at the level of the rectus abdominal muscles through careful central undermining ( Fig. 1 ) combined with selective liposuction. Individualized marking is done preoperatively according to the patient’s individual anatomy. Some areas will have deep liposuction, others superficial and deep, depending on the proximity of the perforators and the areas to be defined. The preservation of Scarpa fascia brings important benefits to the procedure.
Surgical technique
Patient Selection
Ideal patients for the procedure have body mass index (BMI) less than 30, presenting lipodystrophy with abdominal skin laxity. Special attention is given to postbariatric patients (poor skin retraction capability); patients who smoke; and patients who have undergone previous abdominal surgery, including previous abdominal liposuction. Abdominal hernias scars are searched for and noted. These patients may be more amenable for more traditional LAP without definition.
When anatomic definition is done it is important to understand that not every patient will get a high-definition procedure. Most will get a moderate- or even low-definition procedure, depending on BMI, skin quality, and abdominal wall musculature. Because of the variability in patient body type a specific end point in liposuction is hard to define and an artistic point of view combined with an eye on safety is needed. In general, BMI greater than 27 and poor skin quality mitigates against significant definition. Instead, just the creation of a soft negative concavity, especially in the central area, avoids an artificial appearance and results in a better accommodation of the undermined skin flap.
Marking of the Abdominal Flap and Liposuction Areas
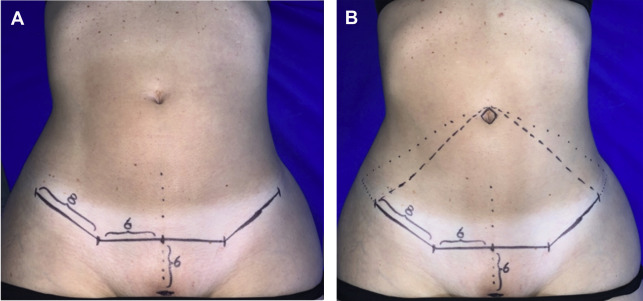
Marking is done preoperatively by drawing a 12- or 14-cm horizontal suprapubic line depending on patient pubic area width that is 5 to 7 cm from the vulvar commissure. Two oblique lines of 7 to 8 cm each are drawn in the direction of the iliac crest within the bikini line completing the inferior incision line; this distance may be longer depending on patient BMI and degree of skin laxity. Next, the supraumbilical limit of the abdominal flap to be resected is marked joining it with the lateral limit of the inferior line ( Fig. 2 ).
With the patient lying down rectus anatomy is delineated. The patient is asked to contract the abdominal musculature and the medial and lateral borders of the rectus abdominis muscle are marked as a red area ( Fig. 3 ). Thus the diastasis is delineated. The costal margin is also marked.
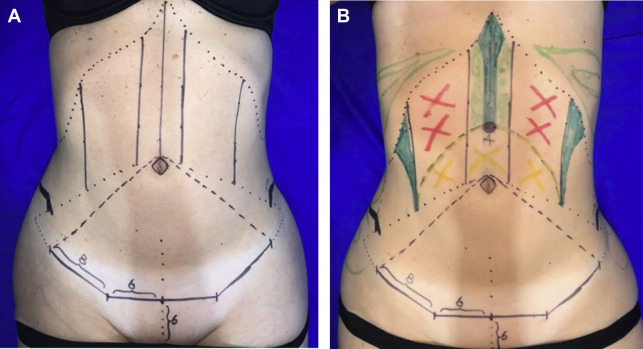
Three lines are designed for a deep and superficial liposuction (dark green lines): the medial line in the supraumbilical abdomen (linea alba), an inverted subcostal triangle as an abdominal line at the junction of lateral borders of the rectus, with the external oblique muscles (semilunaris lines) ( Fig. 4 ). It is important to confirm these lines with the patient in the standing position and with gentle traction of the abdominal flap.
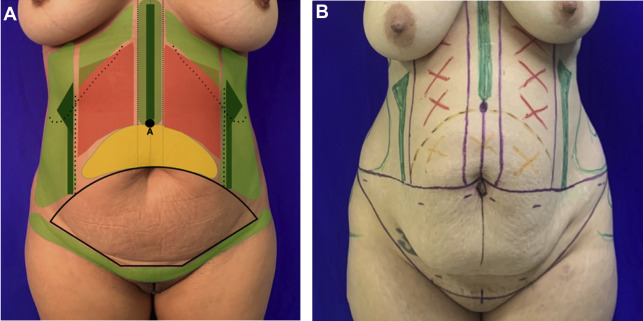
The location of the new umbilicus is marked approximately four fingers above the original umbilicus corresponding to 8 to 10 cm above the pubis (point A, Figs. 3 B and 4 A). The area below (yellow area) is a reference line used to avoid overly aggressive liposuction because this will be the infraumbilical region of the abdominal flap (see Fig. 4 ).
Finally, the demarcation of the pubic area, flanks, iliac crest, or dorsal region if necessary (light green areas) is performed.
Infiltration
Super wet technique is used, infiltrating all the abdominal region with saline solution and adrenaline (1:500,000), between 1 and 2 L in the abdominal area, prioritizing the areas where more intense liposuction will be performed. The incorporation of an infiltration pump and cannulas can significantly diminish the infiltration time ( Fig. 5 ).

Liposuction
Liposuction starts with the patient in the lateral decubitus if dorsal liposuction is performed. The patient is then turned to the opposite lateral decubitus position. First liposuction is made in the dark green areas (areas to be defined), starting in the central region or the linea alba (between the medial edges of the rectus abdominis muscles) and over the position of the new umbilical pedicle (point A, see Figs. 3 B and 4 A). This is done using conventional cannulas of 3 and 4 mm removing fat first from the superficial layer and then from the deep layer. This is repeated in the semilunaris lines and in the subcostal inverted triangle shape, avoiding the trauma of the subdermal plexus. This is done using cannulas with blunt holes facing down or laterally and leaving a soft transition to the surrounding areas ( Fig. 6 ). The end point is to get a pinch test close to 1.5 cm depending on patient BMI, skin quality, and musculature ( Fig. 7 ). The horizontal lines of the rectus abdominis or any other horizontal line are not defined, because when the flap is pulled inferiorly these lines may not be exactly in the anatomic area of the muscle, which may compromise the vascularization of the flap.

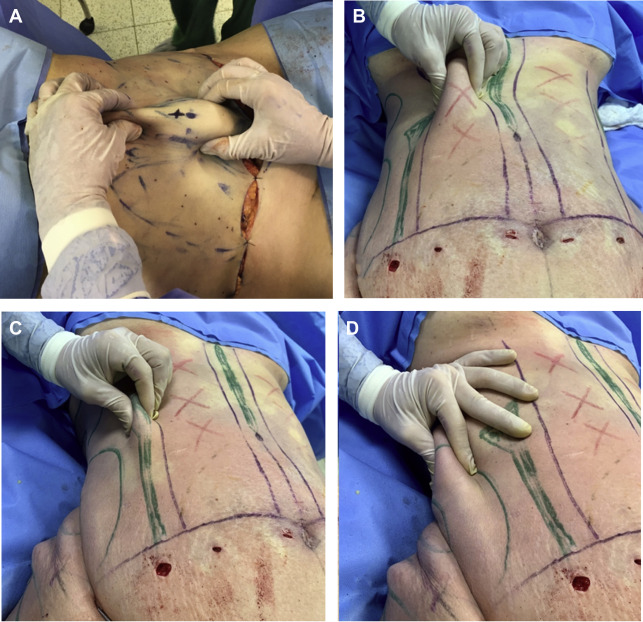
Liposuction in the light green areas (flanks, and any posterior areas) is performed in the deep and sometimes superficial layers until achieving a more natural and harmonious outline of the abdominal wall. The pinch test should be between 1.5 and 2 cm (see Fig. 7 ). This new concept of selective liposuction aims to define the natural curves of the abdomen, accentuating areas of muscular insertions. This concept has previously been described by Hoyos. Unlike Hoyos we perform selective liposuction, not as aggressive as in the high-definition technique. Instead we aim to establish a natural contour and curves of the abdomen, avoiding the stigma of muscular hypertrophy. We also avoid the use of ultrasound-assisted liposuction. It is our preference to use traditional liposuction, although recently we have begun to use power-assisted liposuction.
Next, liposuction of the red area is done in a deep and controlled way, trying not to injure any perforators of the rectus abdominis. Deep liposuction is done in the yellow area. The pinch test should be between 2.5 and 3 cm, superficial, and some deep fat is also maintained because at the time of resecting the abdominal flap the remaining fat in this area can be resected directly, avoiding excessive trauma to this distal flap region (see Fig. 7 ).
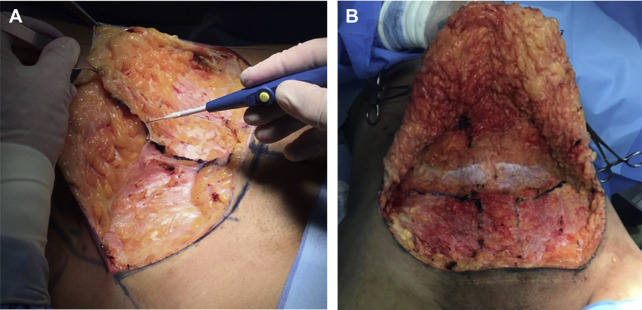
Scarpa Fascia Preservation
The incision of the abdominal skin is done until it reaches the Scarpa fascia, and then the undermining is performed in the suprafascial plane until the level of the anterosuperior iliac spines. This modification on the amount of Scarpa fascia left behind (previously left to the level of umbilicus) was based on the studies and theories of lymphatic preservation, pubic suspension, scar shortening, dead space coaptation, and seroma prevention mentioned in the literature, without creating an inferior abdominal bulge. The dissection then continues in the plane of the muscular aponeuroses to the level of umbilicus, under which no liposuction is performed ( Fig. 8 ).