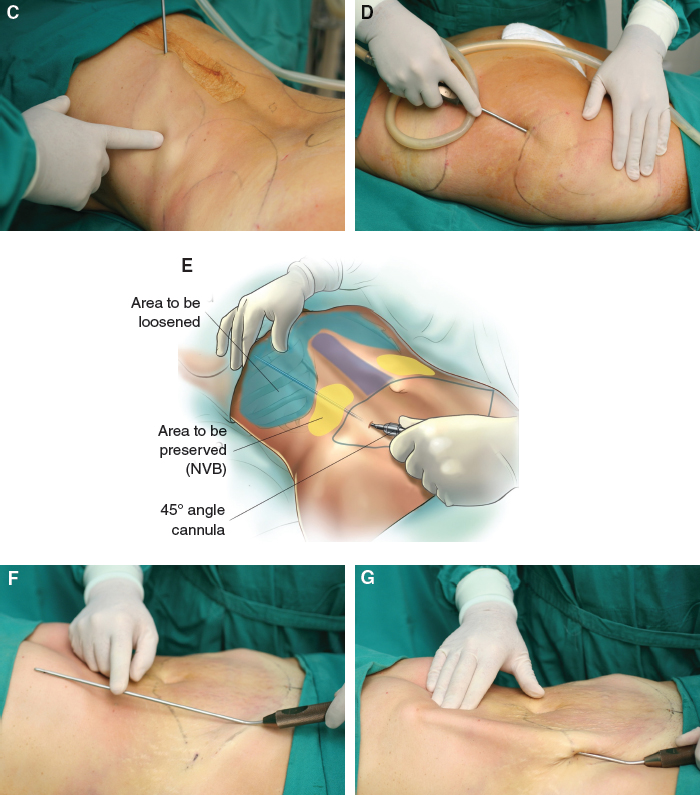
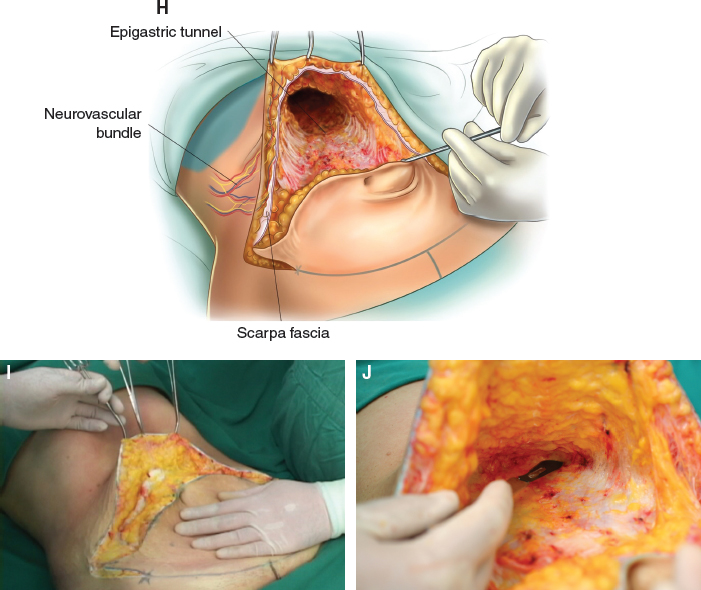
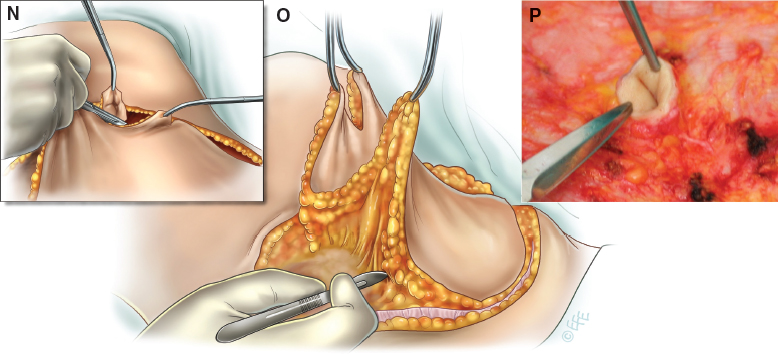
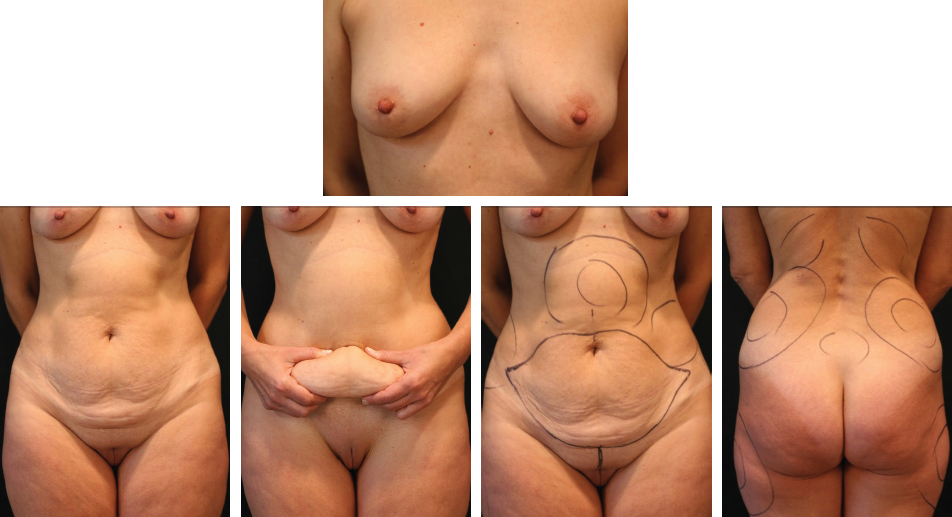
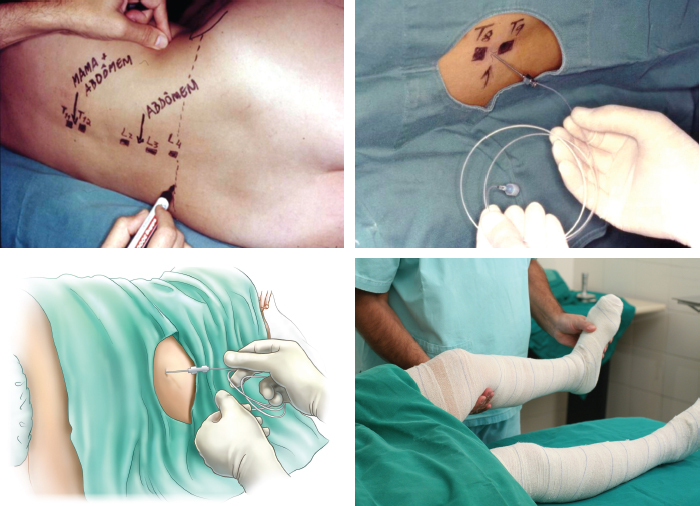
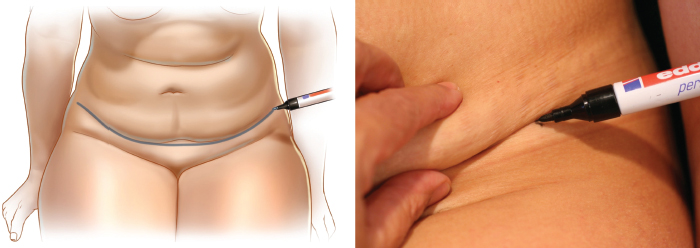
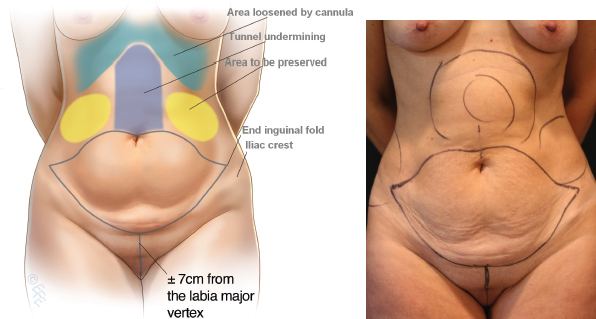
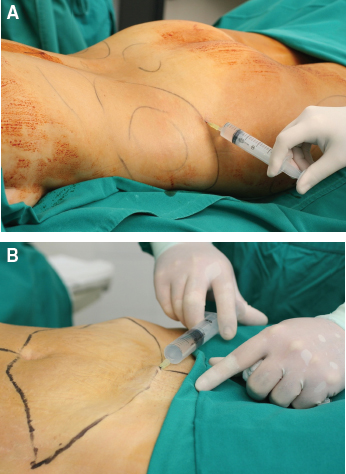
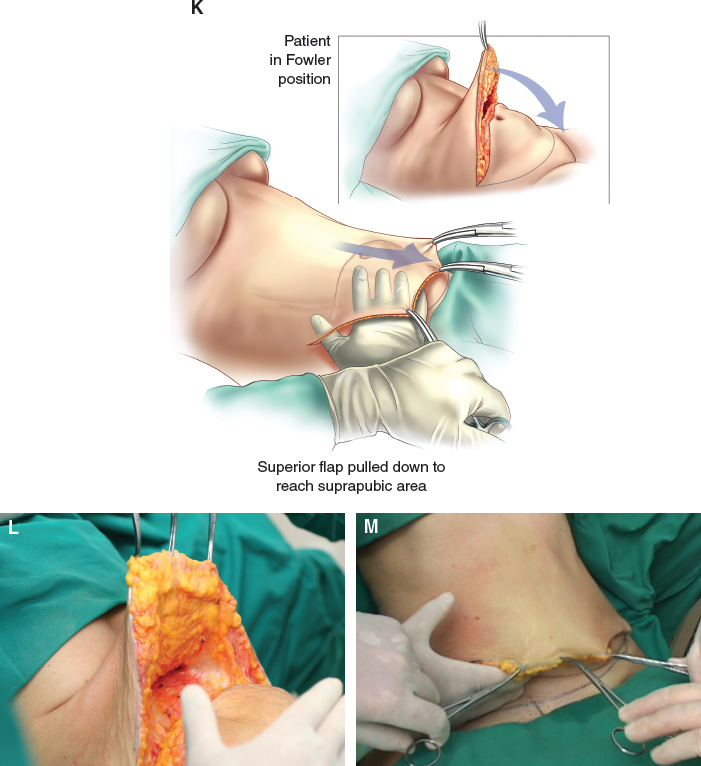
CHAPTER 5 In this chapter, we will address abdominoplasty in combination with mammaplasty, primarily for patients with abdominal laxity, rectus muscle diastases, localized lipodystrophy with breast ptosis, hypomastia, or breast hypertrophy. These are very common conditions among women after pregnancy or after massive weight loss. Breast augmentation, mastopexy, and breast reduction can be frequently be combined with abdominoplasty. For breast augmentation, we prefer to use textured silicone prostheses. For mastopexy, we use the technique described by Pitanguy with a superior pedicled flap. For breast reduction, we prefer the Neto dermoglandular rotation flap, which was described in 1976. Many other techniques have been described in the literature, but these are my preferences; they are very simple techniques that offer good physiologic and aesthetic results. In this chapter, we introduce certain important approaches and details involving these techniques that will help to ensure successful postoperative results. The surgeon must have thorough knowledge of the anatomy of the abdominal wall. The arterial supply is from the inferior and superior epigastric vessels and from the vessels of the flanks. Innervation follows the arterial and venous system from the flanks. Thus undermining must proceed with great care in these areas as well as in the tunnel, and then we shall reach the supraepigastric area approaching the xiphoid process. The lymphatic vessels and myocutaneous nerve branches localized in the inguinal folds and beneath the Scarpa fascia should be considered every time for protection in the excision of the infraabdominal flap. If we damage those branches, numbness in the thighs can result. ■ Costochondral wedge: When performing liposuction of the abdominal wall, it is essential to avoid damaging this area with cannulas. An abrupt maneuver can perforate the wall and damage the hepatic or gastric system. ■ Lateral flanks: The neurovascular bundles emerge from this area and provide arterial and venous support to the abdominal flap. Undermining should not extend into the flanks. ■ Epigastric area: To elevate the superior flap, it is important to undermine a tunnel 6 to 8 cm wide that reaches to the xiphoid process. ■ Suprapubic area: The inferior incision line should be approximately 7 to 8 cm superior to the vertex of the labia majora vertex. About 5 cm of Scarpa fascia should be retained to be affixed to the suprapubic abdominal fascia and to preserve the lymphatic vessels. In an abdominoplasty the most important result is to correct the rectus diastasis to restore anatomic and physiologic normality. The plication of this diastasis can decrease the abdominal circumference in the waist by approximately 6 to 8 cm. In women who have had more than two or three children umbilical hernia is common and should be corrected during the same procedure. Temporary numbness can sometimes occur in the suprapubic area as a result of the stretching associated with the procedure. Fortunately, this numbness typically disappears within 2 or 3 months. The most frequent pathologic indications for abdominoplasty include abdominal laxity with striae, rectus diastases, and an umbilical hernia. Laxity is likely to occur following pregnancy, intensive weight loss, and postbariatric surgeries. We do not operate on patients with a BMI above 30, and smokers need to cease smoking 3 months before surgery. Surgery on individuals with chronic lung diseases such as chronic obstructive pulmonary disease (COPD) is contraindicated unless the pulmonologist determines that the patient is in good enough health to undergo the abdominoplasty. A history of thromboembolism should be thoroughly evaluated, and it is recommended that anticoagulants be given during the postoperative period. During the initial preoperative consultation, we take 10-megapixel digital preoperative photographs from multiple angles with the patient standing to help assess the patient’s deformity. The planned incision lines are marked on the breast and the abdominal wall. The areas to be treated with liposuction are also marked, and the amount of skin and breast tissue to be removed is estimated. Then, with the patient sitting, the amount of skin and fat to be removed from the abdominal wall is estimated. These guidelines should be followed in planning the design of the abdominoplasty: ■ Mark the inguinal folds ■ Mark the suprapubic line 6 to 8 cm from the labia majora vertex ■ Always start the incision in the supraumbilical epigastric area ■ Epigastric undermining should be tunneled to approximately 8 cm wide ■ Transfer patient to Fowler position so the superior flap reaches the pubic area ■ Scarpa fascia should be preserved inside the flap Fig. 5-1 This 42-year-old patient with abdominal laxity, striae, rectus muscle diastasis, and breast ptosis has been marked in preparation for an abdominoplasty combined with liposuction of the designated areas. Fig. 5-2 We usually use high epidural anesthesia. The catheter is inserted in the spinal space between thoracic vertebrae 11 and 12 and is connected to a continuous infusion pump. A 15 ml solution of 7.5 mg/ml of ropivacaine hydrochloride (Naropin) and 30 mg of sufentanil citrate is infused into the epidural space, and an analgesic solution is prepared for postoperative administration by the infusion pump (100 mg of sufentanil citrate and saline solution 0.9%, with 100 ml given at a speed of 5 ml/hr). Compression bandages are placed on the legs to prevent venous thromboembolism. Fig. 5-3 As described previously, with the patient in a sitting position, we mark the estimated amount of skin to be resected. We identify and mark the lateral inguinal folds, and a low abdominal curved line is delineated approximately 6 to 8 cm from the labia majora vertex. A periareolar incision is outlined for the inclusion of breast prostheses. Fig. 5-4 With the patient standing, a line is drawn from the superior umbilical fold and is connected to both lower extremities. The areas to undergo lipodystrophy are outlined. The operation begins with the patient in a supine position. However, when liposuction of the dorsum is indicated, the patient is placed in a prone position before abdominoplasty. We scrub and apply antiseptic solution to the entire abdomen wall and place sterile drapes around the surgical area. Fig. 5-5, A and B Tumescent infiltration and assisted liposuction are performed next. All areas to be lipoaspirated and undermined are infiltrated with a saline solution that only contains epinephrine at a 1:500,000 concentration to avoid excessive bleeding. All local adiposities from the dorsum and flanks are treated with assisted liposuction (suction-assisted lipectomy [SAL]) with a 3 mm cannula. The patient is then rotated to the supine position, and extensive liposuction is performed on the entire abdomen and the epigastric area. It is important to reach the inframammary region and the xiphoid process, even extending to the costochondral border to fully loosen this area. The patient is then rotated into the supine position, and extensive liposuction is performed on the entire abdomen and the epigastric area. It is important to reach the inframammary region and the xiphoid process, even extending to the costochondral border to fully loosen this area. For this maneuver, we use an angular cannula (P. Ragazzo, personal communication, 2013) to prevent internal perforations. The superolateral flank is the only region to be avoided to prevent damage to the neurovascular bundles that give arterial, venous, and neural support to the flap. The supraumbilical skin is released with the liposuction cannula, using the maneuver originally described by Saldanha and Avelar. An incision in the supraumbilical area is then made. A supraaponeurotic undermining is performed in the entire infraumbilical area, and the undermining is continued by a narrow tunnel in the supraumbilical region toward the xiphoid process. The patient is placed in Fowler position, and the abdominal flap is pulled down to assess whether it will reach the suprapubic line. This maneuver is important to ensure an accurate estimate of the amount of skin to be resected without excessive skin tension. This is a safety measure to prevent excessive tension and undesirable vascular complications. The umbilicus is circumcised and a block resection of the entire infraumbilical flap is performed. The new position of the umbilicus is marked in the abdominal flap and an incision is made to pull the umbilicus through the newly created orifice. Quilting sutures are placed, and long-term absorbable intradermic sutures are used to close the abdominal skin. Fig. 5-5, K-M The patient is placed in Fowler position, and the flap is pulled down to try to reach the inferior suprapubic line delineated previously and to estimate whether the inferior flap resection can be performed en bloc without problems. This maneuver is critical to determining whether the defect can be closed without excessive tension. The inferior suprapubic line can then be moved up or down, depending on the laxity and elasticity of the skin and the patient’s biotype. Normally, this is approximately 7 to 8 cm from the labia majora vertex.
Lipoabdominoplasty Associated With Mammaplasty
Surgical Anatomy
Physiologic Considerations
Indications and Contraindications
Preoperative Planning and Preparation
PATIENT EVALUATION
– 5 cm of Scarpa fascia should be preserved in the suprapubic area to protect lymphatic vessels and myocutaneous nerves
Surgical Technique
ANESTHESIA
MARKINGS
PATIENT POSITIONING AND PREPARATION
TECHNIQUE
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine