Summary
The lip has significant functional and aesthetic requirements.
The upper and lower lips are different in both function and anatomy.
The lower lip is somewhat featureless, while the upper lip has significant anatomic components including the philtral columns and Cupid’s bow.
Vermillion alignment is critical, as well as maintenance of the oral commissures.
18.1 Algorithm for Closure
18.1.1 Anatomy
There are significant functional and aesthetic issues in lip reconstruction (▶ Fig. 18.1 and ▶ Fig. 18.2). It is important to understand the functional significance of the upper and lower lips. It is also necessary to realize that the upper and lower lips have very different functional and aesthetic requirements. The lower lip is most important in maintaining a “dam” effect to maintain oral competence, and reconstruction techniques that maintain the muscle integrity of the lower lip are more useful than simply reconstruction with atonic tissue (e.g., free radial forearm flap). The lower lip is actually easier to reconstruct as it is somewhat featureless and tension on closure results in less deformity than tension on closure in the upper lip. Conversely, the upper lip has significant anatomic features that must be maintained or re-created for a successful reconstructive outcome. These anatomic features include the white roll, the philtral column, and Cupid’s bow. 1
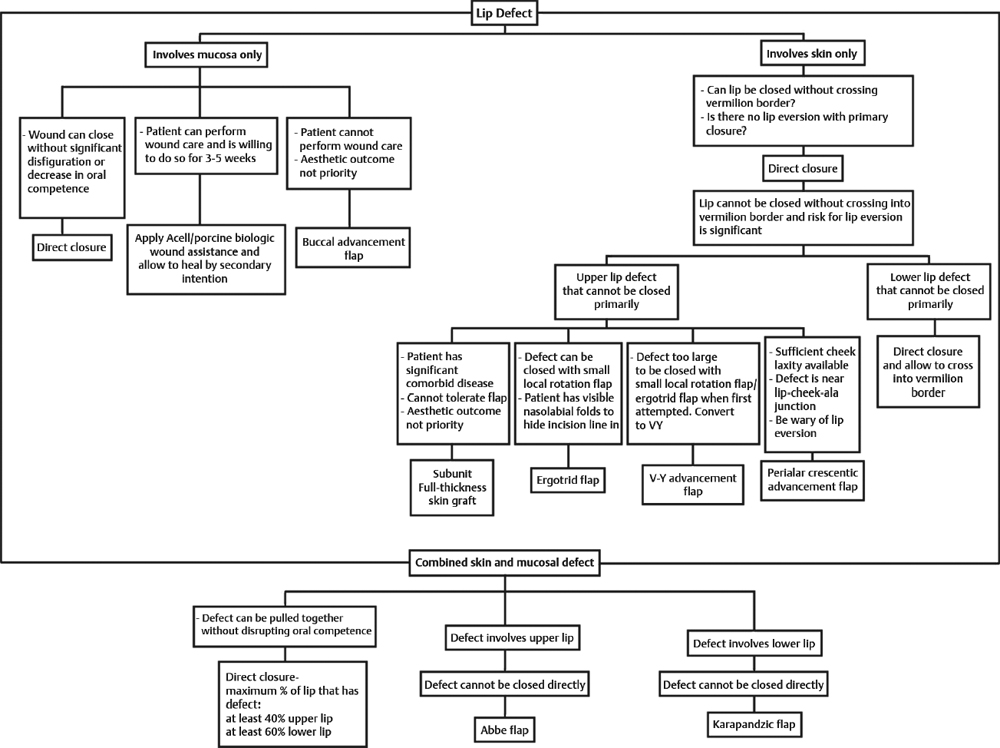
Fig. 18.1 Algorithm for lip reconstruction.
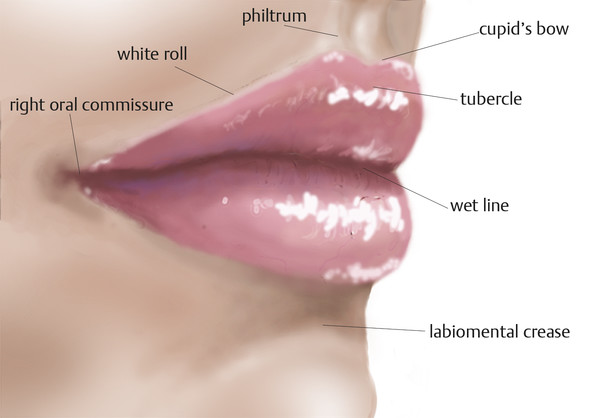
Fig. 18.2 Side lip anatomy.
Generally, reconstruction of the lips should allow for retention of oral competence, preservation of oral commissures, maintenance of vermilion alignment, and prevention of microstomia. These considerations are critical to a functional aesthetic reconstruction. Wounds of the lip are classified into three separate types of defects that include mucosal-only defects, skin-only defects, and then combined skin and mucosal defects. These are each managed quite differently.
18.2 Commonly Applied Methods of Closure
Mucosa-only defects: Delayed healing/secondary intention with or without wound healing agents (i.e., acellular dermal products) and buccal advancement flaps.
Skin-only defects: Direct closure, ergotrid, and V-Y advancement flaps, perialar crescentic advancement flap, and full-thickness skin grafts.
Combined skin and mucosa defects: Direct closure with or without wedge resection, Abbe and rotation flaps, advancement closure, the innervated mucosal advancement flaps, and Karapandzic flap.
18.2.1 Mucosal-Only Defects
Delayed Healing/Acellular Adjuncts
For mucosal-only defects, if primary closure for small-sized defects without lip distortion is a possibility, this should be how the wound is treated; however, the vast majority of these are now managed with secondary intention healing, either with or without acellular matrix or simple porcine acellular dermal matrix (ADM) coverage. 2 There are textbook chapters written on vermilion-only lower lip reconstruction that really ignore the tremendous ability of the lower lip to spontaneously heal without scarring and it is very rare for a vermilion-only defect to heal with a contracture that will distort the lip. 3 Primary management for even large defects of the lower lip are to place ACell matrix powder and then sew in an overlying acellular dermis sheet and then send the patient home with instructions to just keep the surface wet with three to four times daily applications of Surgilube water-based surgical ointment. Gratifyingly, these will uniformly heal well with no late contracture 3 (▶ Fig. 18.3).

Fig. 18.3 A 73-year-old white male status post-Mohs excision for basal cell carcinoma at lower lip. Wound was allowed to heal secondarily. Results shown at 2 months.
Buccal Advancement Flap
There is a role for buccal advancement flaps in cases when patients are unable to provide local wound care or endure the 3 to 5 weeks required for secondary healing. A buccal advancement flap is particularly useful on the lower lip and takes advantage of the laxity present in this region. 4 Great caution must be utilized that the buccal space is not shortened to the point that oral incompetence results. It is also important to understand that a buccal advancement flap that advances the wet mucosa to replace the dry mucosa will never result in a “perfect” lip reconstruction. 4 Secondary intention healing for these cases is preferable (▶ Fig. 18.4 and ▶ Fig. 18.5).
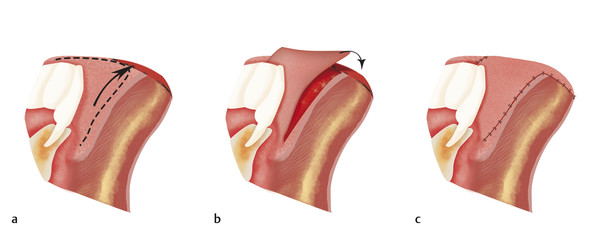
Fig. 18.4 (a) Flap is designed with the leading edge slightly larger than the defect. (b) Flap is elevated and the current wet mucosa is advanced to cover the vermillion defect. (c) Final inset with 4–0 and 5–0 chromic gut sutures.

Fig. 18.5 An 86-year-old female status post complete vermilion excision for multifocal squamous cell carcinoma. Mohs defect closed buccal advancement flap. Postoperative results shown at 4 months.
18.3 Skin-Only Defects
18.3.1 Direct Closure
When approaching skin-only defects, the option of primary closure should strongly be considered first. This approach has significantly changed over the course of the author’s practice, when previously every vermillion-only defect or combined vermillion- and skin-only defect was treated as a wedge excision with excision including the buccal mucosa and then oriented and re-closed. These uniformly resulted in very fine postoperative results as seen in ▶ Fig. 18.5; however, the healing time could often be significant, secondary to the time it takes for the divided orbicularis oris musculature to reapproximate and reinnervate. 5 A much more graded approach with simple linear closure following relaxed skin tension lines is much less invasive and has equal, if not superior, cosmetic results, as seen in ▶ Fig. 18.6. If closure without a significant superior/inferior dog-ear or bunching of the soft tissue is not possible, perform partial debulking of the resultant orbicularis oris muscle to the point of complete excision; however, every effort should be made to maintain the oral mucosa. By providing a watertight seal, it reduces late infection risk and allows for quicker recovery with similar ideal aesthetic appearances 6 (▶ Fig. 18.6 and ▶ Fig. 18.7).

Fig. 18.6 A 38-year-old white female status post-Mohs excision of basal cell carcinoma. Resultant 3 × 4 cm defect was repaired with a complete wedge excision including mucosa and primary closure. Although postoperative results shown at 3 months are good, healing course is significant and current management minimizes tissue resection.

Fig. 18.7 A 47-year-old white female status post 1 × 1 cm Mohs excision of basal cell carcinoma on right upper cutaneous lip. Wound was closed with small dog-ear excision and primary closure. Postoperative results shown at 1 week, 1 month, and 5 months.
Ergotrid and V-Y Advancement Flaps (a Continuum)
Ergotrid flaps, described by Becker, are essentially a rotation advancement flap that takes advantage of the ability to hide the longer advancement limb incision within the nasolabial fold. 7 These can be extended quite far provided patients do have visible nasolabial folds. Their utility in younger patients without well-defined nasolabial folds is significantly less. Every effort should be made to orient the flap to avoid crossing the vermillion border. The ergotrid flap should be considered on a continuum with a V-Y advancement flap for larger, skin-only defects of the upper or lower lip. The incision for the lower limb of the V-Y advancement is outlined and a Doppler is utilized to capture a single perforator, which is sufficient to keep the entire flap alive. 8 First, the ergotrid portion of the superior limb is designed and performed. If there is insufficient advancement, then the lower limb along the white roll is performed and the flap advanced into position for final wound closure, as depicted in ▶ Fig. 18.7. By considering the V-Y advancement flap as a continuum of the ergotrid flap, the surgeon should never be “caught short” on a unilateral upper lip defect as the V-Y advancement flap can repair the entire subunit 8, 9 (▶ Fig. 18.8, ▶ Fig. 18.9, ▶ Fig. 18.10, ▶ Fig. 18.11).

Fig. 18.8 (a) Initial surgical plan is ergotrid flap. Note standing cone excision planned along white roll of lip. (b) Ergotrid flap will not fully cover defect. (c) Incision planned along lower portion of ergot rid to complete V-Y advancement. (d) Ergotrid is converted to V-Y advancement flap. (e) Final postoperative appearance.

Fig. 18.9 A 62-year-old female status post 2 × 1 cm Mohs excision of left upper cutaneous lip for basal cell carcinoma. Wound was closed with small ergotrid flap. Postoperative results shown at 1 week, 2 months, and 9 months, from left to right.

Fig. 18.10 A 70-year-old white male status post 3 × 2 cm Mohs excision of melanoma in situ of left upper cutaneous lip. Wound was closed with V-Y advancement flap. Postoperative results shown intraoperatively at 1 and 5 months, from left to right.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


