CHAPTER 5 Latissimus Dorsi Flap Breast Reconstruction
Key Points
Latissimus dorsi (LD) myocutaneous flaps, first described by Tassini,1 have been used in various reconstructive procedures for decades. In the setting of immediate or delayed breast reconstruction2 LD flaps have several characteristics that can make them excellent options.
Patient Selection
Patients who have undergone radiotherapy can also benefit from the use of an LD flap in breast reconstruction. In these patients, the skin island of an LD flap can replace the constricted, irradiated skin of the breast; and the muscle of an LD flap can cover an implant, thereby decreasing the risk of capsular contracture and implant infection.3–5 Patients who are at an increased risk of mastectomy skin flap necrosis, such as tobacco smokers, may also benefit from an LD flap, which can provide additional muscle coverage of a tissue expander or implant and a robust skin paddle. Furthermore, focal skin and soft tissue defects caused by previous partial mastectomy and radiotherapy that cannot be corrected with implants alone often can be repaired with an LD flap.6,7
Indications
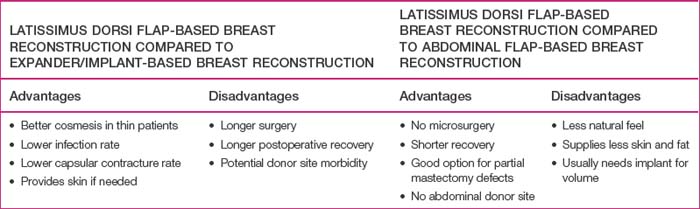
Every patient who desires breast reconstruction must undergo a thorough history and examination to help determine which reconstruction technique should be used. Specific details should be obtained regarding previous surgery to the abdomen, chest and axilla, previous history of radiation, and the patient’s preference for reconstruction method and willingness to undergo major surgery. Many reconstructive surgeons prefer abdominal flaps such as transverse rectus abdominis myocutaneous, deep inferior epigastric, or superficial inferior epigastric artery flaps for autologous tissue-based breast reconstruction. However, patients may not desire or have adequate tissue for an abdominal flap harvest. Furthermore, previous abdominal surgeries such as abdominoplasty, laparotomy, or liposuction may reduce the reliability of an abdominal flap or preclude abdominal flap-based breast reconstruction. In such cases, an LD flap offers a reliable alternative to an abdominal flap. In addition, if an implant is going to be included in the reconstruction, using an LD flap over the implant can improve the contour of the reconstructed breast,8 particularly in thin patients, in whom implant-based reconstructions tend to have less esthetic results (Table 5.1).
Operative Technique
Preoperative evaluation and markings
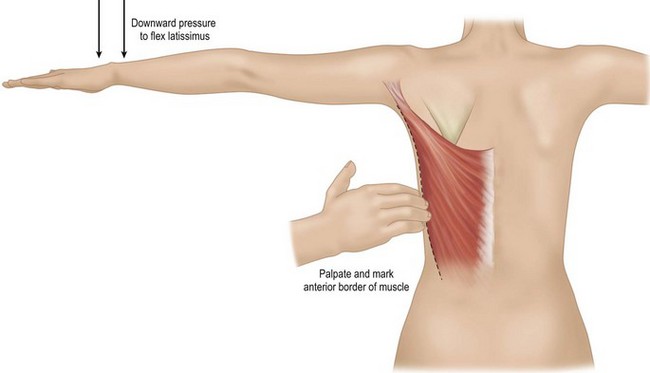
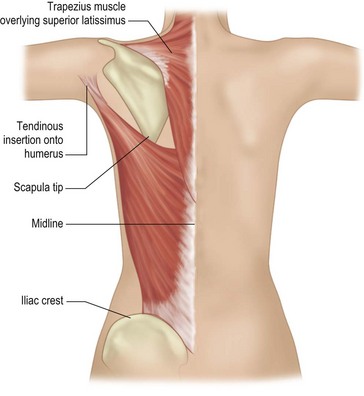
While the patient is awake and standing or sitting upright, the reconstructive surgeon uses a provocative maneuver to evaluate the contractility of the LD muscle (Fig. 5.1). The patient adducts her arm; as the LD muscle contracts, the reconstructive surgeon palpates and marks the muscle’s anterior border. The tip of the scapula, posterior iliac crest, and midline are also marked to further delineate the muscle’s topography (Fig. 5.2). If the patient has a history of lymph node sampling and the LD muscle does not contract when the patient adducts her arm, the thoracodorsal nerve may be injured or transected, and the adjacent thoracodorsal vascular pedicle may also be injured.
If the breast reconstruction requires a skin island, the reconstructive surgeon can design and transpose a template of the size, shape, orientation, and location of the anticipated skin island onto the skin that overlies the LD muscle. The location of the anticipated skin paddle is critical in determining the relative location of the muscle and skin island in the reconstructed breast during inset. The template should also reflect the 90–110° of rotation the flap will undergo from the patient’s back to her chest during the reconstruction (Fig. 5.3). Attaching the template to a towel and using the axilla as a pivot point can help the surgeon confirm the flap will reach its intended final location. To ensure that the flap donor site can be closed primarily, the reconstructive surgeon should pinch together the anticipated incision lines. In most patients, primary closure without significant tension can be performed if the skin island is less than 10 cm wide. If a skin island is not required for breast reconstruction, the reconstructive surgeon can harvest the LD flap through a small incision in the posterior axilla and use endoscopy to limit the number of incisions made on the patient’s back.

Flap elevation
Full-muscle myocutaneous flap elevation
If the patient has undergone axillary lymph node sampling, the reconstructive surgeon should identify the vascular pedicle anteriorly though the mastectomy defect while the patient is supine. Once the pedicle has been identified and preserved, the reconstructive surgeon should mobilize the flap as much as possible from the surrounding soft tissues (Box 5.1).
Box 5.1 Surgical steps in latissimus dorsi (LD) flap harvest
Related posts:
 Gluteal Flap Breast Reconstruction
Gluteal Flap Breast Reconstruction
 Surgery of the Breast in Poland’s Syndrome
Surgery of the Breast in Poland’s Syndrome
 Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
 Autologous Flap Use in Breast Reshaping after Massive Weight Loss
Autologous Flap Use in Breast Reshaping after Massive Weight Loss
 Fat Injections to the Breast: The Lipomodeling Technique
Fat Injections to the Breast: The Lipomodeling Technique
 Subfascial Breast Augmentation
Subfascial Breast Augmentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


