Flap |
|
Tissue |
Muscle or musculocutaneous flap, pedicle or free |
Course of the vessels |
From the axilla along the anterior border of the muscle: it enters the muscle from underneath and then spreads into the three major branches at the undersurface of the muscle |
Dimensions |
Can be tailored to almost any size; maximum dimensions, 20 × 35 cm |
Extensions and combinations |
Can be raised as muscle, musculocutaneous, and perforator flap; combinations are possible with any component from the subscapular system (i.e., bone, skin, fascia, or muscle) |
Anatomy |
|
Neurovascular pedicle |
Thoracodorsal artery |
Artery |
Usually one vein that originates from the subscapular vein |
Veins |
Up to 15 cm; branches of the subscapular system; anatomical variations in 3–5% of population |
Length and arc of rotation |
Artery, 2–4 mm; vein, 2–5 mm |
Diameter
Nerve |
Motor nerve; some studies report deep sensation 18 months after coaptation to the sensory recipient |
Surgical technique |
|
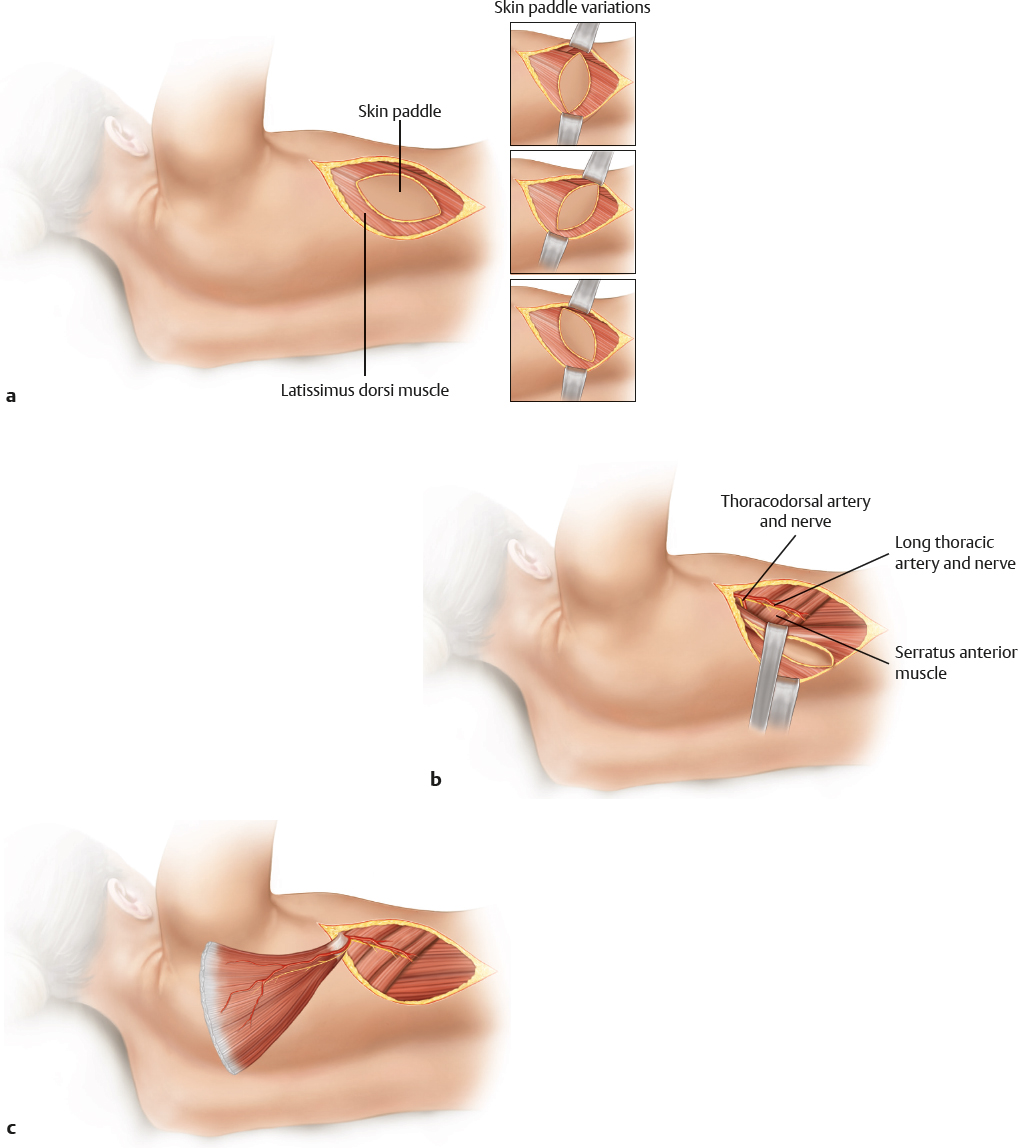
Preoperative examination and markings |
No vessel identification necessary; in cases of previous axilla dissection or radiation, check muscle function; if muscle function is intact, vessels are usually not violated; mark the anterior muscle border and the tip of the scapula to outline the flap borders |
Patient position |
Midlateral; arm elevated 90 degrees |
Dissection |
Mark the flap dimensions; start with an incision along the muscle border; identify the muscle border and branch to the serratus muscle; identify the pedicle and follow the pedicle to its origin; free the anterior border of the muscle and raise the flap from ventral to dorsal toward the spine; take care to coagulate or ligate the perforating vessels; divide the muscle distally as required; divide the muscle at the spine insertions; raise the muscle in a cranial direction; ligate the serratus branches; check perfusion; divide the pedicle |
Advantages |
|
Vascular pedicle |
Long and reliable; large-caliber vessels |
Flap size and shape |
Any flap size is possible: the latissimus dorsi is the largest muscle in the body |
Combinations |
Numerous combinations are possible, including multicomponent flaps with other flaps from the subscapular system; vascularized bone can be harvested as rib grafts with the latissimus dorsi or on a connected pedicle from the scapula; fascia can be added from the serratus muscle |
Further options |
Scapular flaps are still available if the latissimus dorsi is harvested correctly; the serratus muscle is available, but vessels are small |
Disadvantages |
|
Bulkiness |
Muscle can be bulky; skin islands in musculocutaneous flaps are usually bulky and require secondary contour correction |
Donor site morbidity |
Donor scar is rather conspicuous; approximately 7% loss of shoulder function |
Pearls and pitfalls |
|
Dissection |
Watch out for constant large perforator vessels at the tip of the scapula (ligate); finalize the dissection of the pedicle by splitting the fascial leaf, which separates the latissimus dorsi from the teres muscles dorsally; ligate the branch to the scapula, and do not confuse it with the second branch to the muscle; take a skin island as a monitoring island, if desired. |
Extensions and combinations |
Dissect the pedicle up to the axillary artery to rule out anomalies of the vascular system so that all components are nourished by one pedicle; if there are anomalies, the operative strategy has to be adjusted to perform additional microanastomoses |
Contouring and correction |
Muscle flaps usually shrink, and contouring is required in approximately 50% of cases; musculocutaneous flaps almost all tend to sag and need contouring; in the case of functional muscle transfers, readjusting muscle tension is sometimes required |
Clinical applications |
Coverage of large surface area defects; functional free muscle transfer for loss of forearm flexor and extensor systems; pedicle muscle transfer for restoration of biceps function |