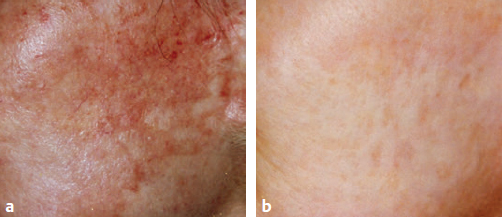
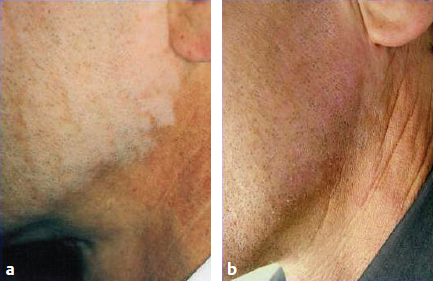
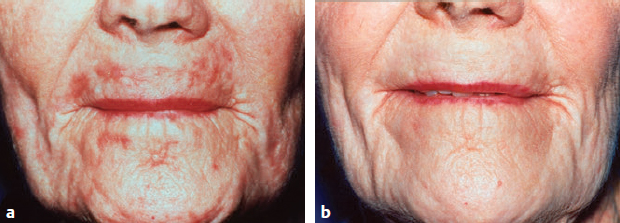
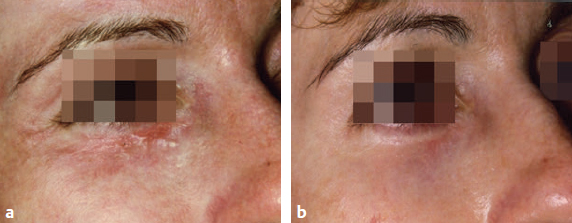
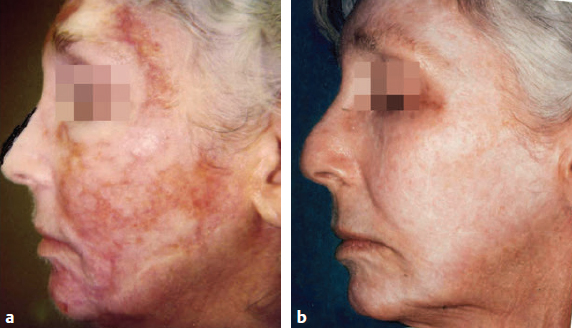
CHAPTER Over the past two decades, laser facial resurfacing has served as a valuable method toward the goal of achieving facial rejuvenation. The ability to effectively combat the normal and inevitable consequences of aging, such as rhytides, lentigines, alterations in skin texture, and scarring, remains paramount, and practitioners are always searching for effective nonsurgical means. Luckily, many advancements in laser technology have been made since the relatively primitive ruby and CO2 lasers were developed in the early 1960s, and new technologies have increased efficacy while minimizing adverse effects.1 Four broad categories of laser resurfacing have formed from such innovations. These consist of the novel ablative nonfractionated type, the less dramatic but undeniably safer nonablative nonfractionated type, the hybrid nonablative but fractionated type, and the ablative fractionated type used by carbon dioxide (CO2) and erbium-doped: yttrium aluminum garnet (Er:YAG) systems. Although some of these categories of lasers maintain higher safety profiles over others, all types of ablative treatments have a risk for complications. When discussing laser resurfacing, understanding the fundamental differences between these categories is essential. The term nonablative refers to a treatment that selectively and often minimally damages the dermal tissue while sparing the epidermis, achieving less dramatic results, but maintaining a higher safety profile. This is in contrast with ablative lasers, which essentially vaporize the epidermal layer while stimulating the dermis, necessitating far more downtime and a more difficult recovery but achieving significantly superior results. The term fractionated refers to the ability of the laser to target a specific proportion of treated skin, creating discrete and separated columns of affected tissue instead of acting on the entire skin surface. This allows the surrounding untreated skin to contribute to the healing process through epithelial migration.2,3 Although the exact biochemical processes by which laser resurfacing acts to improve cosmetic appearance are still not fully determined, the relationship between the wavelength that the laser emits and a high absorption coefficient for tissue water is what allows highly controlled thermal damage to the desired skin layer. For example, the CO2 laser emits a wavelength of 10,600 nm, which is strongly absorbed by tissue water. It is hypothesized that through this the CO2 laser targets the appropriate depth in the skin and causes immediate contraction of the ablated area by denaturing existing old collagen.4 Subsequently, new collagen formation is stimulated, and in conjunction with ablation of the epidermis, cosmetic enhancement is achieved over time through controlled wound healing as new epidermal and dermal tissue takes the place of the photoaged and damaged skin. Compared with the CO2 laser, the Er:YAG laser emits light at the 2,940-nm wavelength. At this frequency, the peak absorption range of water is more closely approximated, and as such the Er:YAG laser possesses an absorption coefficient for water 16 times greater than the CO2 laser.2 Despite this, both systems can achieve similar efficacy, especially with the advent of the long-pulse erbium laser. Past comparative studies have shown the Er:YAG laser may cause fewer severe side effects,5 and thus many practitioners have chosen to only use this modality. However, many patients’ desired cosmetic outcome or individual tolerance may not require or allow for ablative laser resurfacing, and nonfractionated and nonablative lasers are still widely used for various indications. Comparatively, ablative laser resurfacing does cause more side effects, and additional minor and occasionally severe complications can occur. The following sections detail potential side effects, complications, and unfavorable results and how best to avoid them. First and foremost, as with any cosmetic procedure, patient selection must only involve individuals who not only possess the ability to thoroughly understand the procedure and its associated risks, but also hold realistic expectations for the end result. Depending on the type of laser used, patients must be able to accept that most ablative laser resurfacing may result in significant downtime and an extended period of recovery. In addition, appropriate screening must be performed so as to exclude those individuals who may lack the diligence or ability to perform adequate postoperative care to prevent complications during the wound-healing stage. Without question, proper wound management is imperative to achieve successful results. Likewise, patients with medical conditions involving poor wound healing, a history of collagen vascular disorders, conditions with propensity to koebnerize, or past facial keloids or hypertrophic scarring may be unfit candidates to undergo laser resurfacing. Recent isotretinoin therapy within 6 months up to a year or a history of radiation within the treatment area should also be considered an increased risk for scarring complications. Although a recent study found that concomitant isotretinoin was safe in an Asian population, I urge considerable caution based on personal experience.6,7 Perhaps one of the most predictable and notable associated complications involving patient selection is those patients with ethnic skin or those with Fitzpatrick types IV to VI. Again, caution and a conservative approach must be observed to prevent postinflammatory hyperpigmentation and other pigmentary changes in these individuals.1 An important consideration for laser resurfacing should be the planned method of adequate anesthesia. Ablative resurfacing in particular causes significant stimulation to dermal nerve fibers, resulting in substantial discomfort and pain. When only small, localized, or superficial areas of treatment are involved, methods such as oral sedation, topical anesthetics combined with or without nerve block, or cryoanesthesia may be sufficient. However, if deep resurfacing of the entire face is planned, additional approaches such as monitored intravenous sedation may be warranted. Injected nerve blocks combined with topical and oral preparations are often preferred, negating the need for supervised anesthesia, but drawbacks include potential tissue distortion, increased procedure time, and inadequate pain control.8 Ultimately, appropriate methods of anesthesia must be tailored to patient tolerance and preference and the comfort level of the provider. The provider must also possess an adequate knowledge of the different capabilities and adjustable settings of the proposed device. All lasers have inherent and adjustable properties such as pulse duration, spot density and diameter, and depth of penetration. Perhaps the most important adjustable parameter is laser fluence, or the laser energy per unit area of tissue. Cosmetic outcome and the rate of complications are significantly related to the fluence and the number of laser passes. Unquestionably, there is a direct relationship between greater fluence, depth of penetration, and number of passes with longer healing time. With the advent of short-pulse and long-pulse Er:YAG lasers, dramatic results and increased coagulation of the dermis that was previously only achieved with CO2 lasers is possible, with the potential benefit of decreased side effects. With fractionated lasers, microspot density is very important when balancing the desired aesthetic results with risk of complications. As mentioned previously, fractionated lasers cause discrete columns of tissue injury, and the degree of fractionation can usually be adjusted. This leaves the surrounding untreated skin with the ability to contribute to the wound-healing process through epithelial migration. In addition, the unaffected areas allow adequate heat transfer and help prevent excessive dermal bulk heating, which has also been proven directly proportional to the rate of complications.3 Finally, an experienced practitioner can increase the effective area of ablation through multiple passes and overlap of pulses, optimizing aesthetic results. Summary Box Side Effects and Complications of Ablative Laser Resurfacing Expected Short-Term Side Effects Erythema Edema Pain Pruritus Minor oozing Minor bleeding Minor crusting Complications Contact dermatitis Acne/milia Viral/bacterial/fungal infection Sharp demarcation lines Persistent erythema Hyperpigmentation Hypopigmentation Hypertrophic scarring Delayed healing Tooth enamel damage Corneal damage Ectropion formation The ideal surgical goal may vary from patient to patient, but minimizing photoaging, rhytids, and scars with as few complications as possible is the ultimate objective. Increasing the effective degree of ablation will cause greater dermal contraction and collagen stimulation, which in turn can generate more dramatic results and improve deeper rhytids, but also carries greater risk of complications. Also, different areas of facial skin have varying levels of tolerance for delivered fluence. For instance, perioral areas and cheeks will traditionally tolerate higher fluences. In contrast, the lateral aspects of the cheeks and the preauricular skin are vulnerable to prolonged erythema and hyperpigmentation, and thus lower fluences should be used. Similarly, although the glabella may require more energy to achieve desired results, the rest of the forehead does not usually require comparative energy. Caution is important around the eyelid skin, but the lateral canthal areas have shown greater tolerance for more aggressive fluences.9 Other areas of the body such as the neck must be approached with extreme care because of the lack of pilosebaceous units, decreased vascularity, and skin thickness; multiple cases of hypertrophic scarring have been reported.10 If only the face is to be resurfaced, sharp lines of demarcation may result, and thus feathering of the neck and hairline should be performed. Sharp transition zones are more often problematic in men, because women are better able to hide abrupt alterations with makeup and foundation. There are many possible short-term side effects with laser resurfacing, and many cannot be prevented, but every effort to prevent further complications should be made. Erythema and edema are inescapable side effects with ablative laser resurfacing and are considered normal reactions to la ser-induced tissue injury. Swelling and edema after resurfacing usually peaks around 2 to 3 days and should resolve within around 1 week. Increased blood flow, inflammation, metabolic activity, and collagen remodeling are likely responsible.1 However, persistent erythema, considered to be erythema which lasts up to 6 months or more, is not common and is most often seen with CO2 lasers as a result of more extensive residual thermal necrosis of the dermis. Other factors that can increase the likelihood of persistent erythema are multiple laser passes, pulse stacking, mechanical abrasion and rubbing of the skin intraoperatively, postoperative infection, and patient susceptibility because of preexisting conditions or therapies. These susceptibilities include a history of rosacea, previous resurfacing or use of acid peels, or use of retinoic acid derivatives.11 Other very common aftereffects witnessed after resurfacing include minor crusting, oozing, and bleeding. Adequate wound care and strict application of petroleum-based products will improve the skin barrier and epithelialization, which in turn promotes more pleasing aesthetic outcomes. When erythema persists and is associated with pruritus, contact dermatitis should be considered, although often it is difficult to distinguish. This is usually irritant as opposed to allergic in nature; recently resurfaced skin is particularly sensitive to topical products and chemicals, and thus sunscreens, ointments, and topical antibiotics should be avoided.12 Proper post-resurfacing wound care consists of liberal application of petroleum-based products such as Aquaphor to the entire treated area. Patients should be instructed to avoid the urge to scratch or irritate the area while the skin is in this vulnerable state. Some studies have shown that occlusive dressings can be used up to the first 4 days after the procedure and may contribute to a decreased incidence of crusting, pruritus, erythema, and postoperative pain compared with controls.13 Others have investigated the use of occlusive silicone dressings, the application of platelet-rich plasma, and even adipose-derived stem cells, all of which showed potential for significant reduction in length of time for erythema and edema and appeared to hasten wound healing.14–16 However, any type of occlusive medium, with a dressing or without, can contribute to the development of infection, acne, and milia, which are very common after laser resurfacing, especially in patients who are already acne-prone. Laser-induced injury to the pilosebaceous apparatus may also occur and contribute to aberrant follicular epithelialization manifesting as acne and milia.11 These flares tend to develop within the first few weeks after treatment for acne-prone individuals, and at around 6 weeks for those without prior history.17 Whether prophylactic antibiotics to prevent postoperative infection are necessary with laser resurfacing is unclear. Investigations into the potential benefit of administering prophylactic doses show a wide array of results and varying recommendations. Bacterial infections during the immediate postoperative phase are likely caused by streptococcal and staphylococcal species. However, fungal infection such as candidiasis has been documented and may be difficult to diagnose because it resembles acne or milia formation. Those at risk for fungal infection include those with diabetes, angular cheilitis, immunosuppression, and vaginal candidiasis.11 Some studies have shown virtually no incidence of bacterial infection with different prophylactic treatment regimens—intraoperative cephalexin and postoperative azithromycin or dicloxacillin.18,19 On the other hand, one study showed the rate of pseudomonal and serratia infections was significantly higher in patients routinely given such prophylaxis.20 As a result, no general consensus exists on the use of prophylactic antibiotics, and many practitioners choose open wound healing combined with vigilant observation for any evidence of infectious process. Any postoperative infection can place the patient at increased risk for permanent scarring and further complications. In contrast with the risk of bacterial and fungal infection, viral prophylaxis against the reactivation of herpes simplex virus type 1 (HSV-1) is almost universally indicated, regardless of previous history. Reactivation of HSV-1 is one of the most common disruptions of proper wound healing and increases the risk of secondary bacterial infection (Fig. 17.1). Because of the incomplete epithelial barrier, classic vesicles are unlikely to form; instead erythematous erosions associated with pain, fever, and malaise may encompass the presentation.21 Reactivation and rarely primary HSV-1 infection is likely secondary to the disturbance of the normal skin barrier and stimulation around mucocutaneous areas by laser damage and trauma. To prevent this complication, adequate prophylaxis usually consists of antivirals such as valacyclovir or acyclovir given at least 1 day before the procedure and usually continued up to 7 to 10 days afterwards.22 Most patients and physicians prefer the use of valacyclovir because of its easier dosing. Serious and concerning complications include dyschromia and altered skin pigmentation, hypertrophic scar development, delayed healing, and ectropion formation. Dyschromia is a well-documented adverse effect after resurfacing and is more common in dark-skinned patients and those of higher Fitzpatrick types because of higher melanin concentration. Because dark skin absorbs electromagnetic energy much better than fair skin, the risk of thermal injury is increased. Moreover, melanin’s wide absorption spectrum of visible light and near-infrared light increases the risks for any laser treatment and can result in permanent complications.23 Hyperpigmentation in fair-skinned individuals is usually a result of excessive sun exposure to vulnerable skin after the procedure.24 Postinflammatory hyperpigmentation is usually transient and relatively common within the first month after laser treatment and will usually resolve spontaneously. In the past, some physicians attempted to prevent hyperpigmentation preoperatively with 6 weeks of skin therapy using topical tretinoin, alpha hydroxy acids, or 4% hydroquinone bleaching cream in an effort to suppress melanocytes, but newer studies have shown no statistical benefit of these practices.21,25 Unlike hyperpigmentation, hypopigmentation witnessed after laser resurfacing is a potentially serious and permanent complication and does not usually manifest until 6 to 12 months postoperatively. It most commonly results from resurfacing performed too deeply into the reticular dermis (Fig. 17.2).24 Particularly susceptible facial areas include those adjacent to photodamaged skin, such as the mandible.11 Because photodamaged tissue is removed, and new nondamaged skin will replace the damaged epidermis and dermis, almost all patients experience some relative hypopigmentation. Despite advances in fractionated technology, caution and conservative treatment is emphasized in darker-toned patients. Fig. 17.1 Bacterial infection 1 week after resurfacing. Fig. 17.2 Hypopigmentation. (a) Two years after resurfacing. (b) After multiple narrow-band ultraviolet A treatments. Scarring, particularly hypertrophic scarring, is also another serious potential complication of laser resurfacing. Multiple factors can influence the incidence of hypertrophic scarring. These include excessive thermal energy to the skin or postoperative bacterial, fungal, or viral infections. Untreated contact dermatitis can also cause hypertrophic scarring. Furthermore, recent use of isotretinoin, a history of keloid formation, and previous radiation therapy can predispose patients to scarring complications.26,27 Particularly susceptible areas are those nonfacial regions with less vasculature and blood supply, such as the neck, chest, infraorbital region, and mandible. The least amount of possible pulse energy, pulse stacking, density, treatment fraction, and laser passes is recommended when treating these areas (Figs. 17.3 and 17.4). The first indicators of potential impending scar formation during the wound-healing phase are focal areas of induration and intense erythema. Immediate recognition is vital to prevent permanent scar development.11 Fig. 17.3 Scarring. (a) Six months after resurfacing. (b) One year after resurfacing after multiple pulsed-dye laser treatments. Fig. 17.4 Scarring. (a) Four months after resurfacing. (b) Six months after resurfacing after multiple pulsed-dye laser treatments. Fig. 17.5 Delayed healing syndrome. (a) Six months after resurfacing. (b) One year after resurfacing after multiple pulsed-dye laser treatments. For reasons not entirely clear, occasionally patients experience great difficulty with healing after laser resurfac ing.28 Associated often but not always with deeper laser procedures, this “delayed healing” syndrome is believed to result from a combination of infection and potentially autoimmune phenomenon that prevents normal reepithelialization. Documented cases usually involve patients with Fitzpatrick type I or II skin, and after a prolonged healing course of around 8 to 10 months, significant scarring is evident29 (Fig. 17.5). Although cosmetic complications are of paramount importance, one functional adverse event requires special attention. Ectropion formation of the lower eyelid is a real concern, especially in patients with a history of previous lower blepharoplasty. A “snap test,” which involves manual downward pull of the lower eyelid, can be used to detect increased risk. If the lower eyelid does not quickly return to its normal resting position within 3 seconds, laser surfacing should not be performed around this area.11 Damage to the cornea and tooth enamel can and should always be prevented with proper protection and metal shielding for the patient. If proper precautions are not taken, tooth enamel may be fractured by the impact of the laser or subsequent heat production.24 When unfavorable results and complications occur, the treatment varies depending on the type and severity of the adverse event and the underlying cause. Proper wound management during the initial healing phase has already been mentioned, and erythema is unavoidable; however, persistent erythema may require treatment to prevent possible scar formation (Fig. 17.6). This can be accomplished by administering a strong class 1 topical corticosteroid. Additional studies have shown that topical vitamin C, also known as ascorbic acid, may decrease postlaser erythema through its anti-inflammatory effects. However, administration of vitamin C should be reserved until reepithelialization has finished, and the risk of irritation to the area may outweigh the potential benefit. When erythema and pruritus worsen, and contact or irritant dermatitis is suspected, a thorough history must be obtained to make sure that the patient has been following all postoperative instructions and that potential irritants such as home remedies, sensitizing topical antibiotics, or other fragrant moisturizers have not been applied. As mentioned previously, patients should be instructed to avoid further mechanical irritation or scratching to the area to prevent further crusting and poor cosmetic outcome. Some patients may require a course of oral antihistamines such as diphenhydramine or hydroxyzine. These can be used in conjunction with cool, wet compresses in addition to mild topical corticosteroids. In some severe cases, systemic steroids may be necessary to control pruritus and inflammation.11
17
Laser Facial Resurfacing
Avoiding Unfavorable Results and Complications in Laser Resurfacing
Patient Selection and Preoperative Planning
Intraoperative Considerations
Postoperative Complications

Managing Unfavorable Results and Complications in Laser Resurfacing
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine