Fig. 10.1
Laparoscopic sleeve gastrectomy (LSG) and duodenal jejunal bypass (DJB)
LSG/DJB may be performed on patients who have fulfilled the bariatric and metabolic surgery indications as well as risk factors of bypassed stomach cancer.
Risk factors of gastric cancer are determined as follows:
1.
Helicobacter pylori (H. pylori) positive
2.
Atrophic change of gastric mucosa, including intestinal metaplasia with or without H. pylori infection
3.
Family history of gastric cancer
10.2 Operative Technique
The patient should be in the supine position, under general anesthesia, with their legs separated. Five trocars are used as seen in Fig. 10.2. The supra-umbilical trocar is for the camera, and the 5 mm port at the subxyphoid is for the liver retractor. Two 12 mm trocars are placed at the left subcostal margin and 10 cm below that 12 mm trocar. A 15 mm trocar is placed at the upper right abdomen to retrieve the specimen. The position of trocars is the same as when performing LSG.
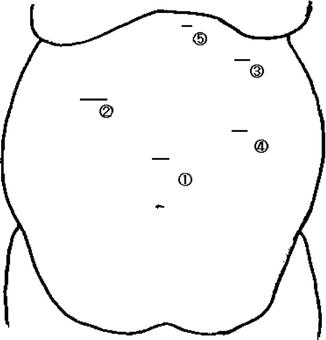
Fig. 10.2
Trocar placement
Regarding the sleeve gastrectomy, the technical aspects are mentioned in another chapter. We will focus on DJB parts in this chapter.
The DJB parts are (1) dissection of the duodenum, (2) jejunojejunostomy, and (3) duodenojejunostomy.
In this chapter, we would like to show the pictures from an outside view to show the readers the position of the surgeon and how the surgery is performed.
10.2.1 Dissection of Duodenum (Fig. 10.3)
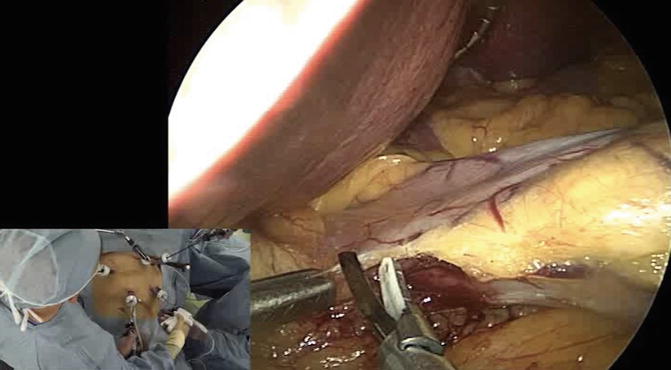
Fig. 10.3
Dissection of the duodenum
For LSG, devascularization of the gastroepiploic artery is usually started from 4 to 5 cm proximal of the pyloric ring. DJB requires a dissection of the duodenum, so that dissection needs to be continued distally to approximately 1.5 cm beyond the pylorus. Instrument palpation is used to confirm the position of pylorus. The retro-duodenal and supra-duodenal tissues are dissected free in order to facilitate transection of the duodenum at this point with a blue or purple cartridge linear stapler. The right gastric artery should be preserved to maintain the blood supply to the anastomosis. Extra care must be taken during this step because an injury to the pancreas posterior to this point may lead to a lethal complication. The wall of duodenum is thinner than that of the stomach, so the surgeon must make sure to avoid a cavitation injury when using the laparoscopic coagulating shears (LCS).
The transection of the duodenum is performed after LSG is completed (Fig. 10.4). We usually put reticulating linear staples from the left lower trocar to transect the duodenum at a right angle to the duodenum. Usually we use a blue or purple 60 mm stapler. If there is bleeding from the staple line, it is helpful to use sutures.

Fig. 10.4
Transection of the duodenum
10.2.2 Jejunojejunostomy
The omentum is displaced cephalad to expose the ligament of Traiz (Fig. 10.5




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
