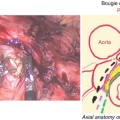
Fig. 6.1
Roux-en-Y Gastric Bypass
1.
Circular stapler anastomosis
2.
Linear stapler anastomosis
3.
Hand-suturing anastomosis
We prefer to perform using the hand-suturing anastomosis method, so the technique described in this chapter is based on LYRGB with hand-suturing gastrojejunostomy, but we would also like to describe all three anastomosis techniques.
6.2 Position of the Patient
The position of the patient completely depends the surgeon’s preference. Many surgeons prefer to use the split-leg position, but others prefer the supine position. Almost all surgeons prefer reverse Trendelenburg position. We use the split-leg reverse Trendelenburg position; the camera assistant stands between the legs and the surgeon stands on the right side of the patient.
6.3 LRYGB Consists of These Manipulations
1.
Trocar insertion
2.
Jejunojejunostomy
3.
Gastric pouch formation
4.
Gastrojejunostomy
5.
Others (including mesenteric closure, leak test)
Sequential order may depend on surgeons’ preference.
6.3.1 Trocar Insertion
For morbidly obese patients, it is very difficult to do “open method” for the first trocar insertion. Initial entry is performed without insufflation using a 10 mm non-bladed optical trocar system. Using a bladed optical trocar system may cause serious injury to the blood vessels and lead to major hemorrhage, so we avoid using a bladed trocar for the first port. The camera is placed at 2–3 cm left from the midline, 18 cm from the xiphoid. Three 12 mm ports are placed at (1) 10 cm from the midline and just beneath the costal margin, (2) 10 cm below that port, and (3) 3 cm right from the midline and 2 cm beneath the right costal margin. One 5 mm port is placed just below the xiphoid to put the lever retractor before formation of the gastric pouch (Fig. 6.2).
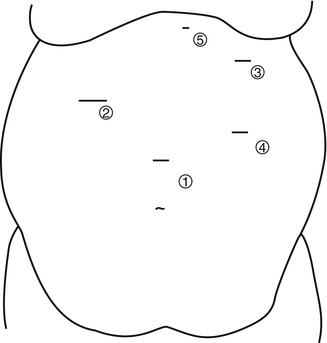
Fig. 6.2
Trocar position
Close attention to the angle of entry of the ports can reduce the resistance of the abdominal wall to the instruments, allowing for a more precise and less fatiguing operation.
6.3.2 Jejunojejunostomy
The omentum is displaced cephalad to expose the ligament of Treitz (Fig. 6.3). The length of the biliopancreatic tract, which means the length from the ligament of Treitz, may be determined by the surgeon’s preference. Usually it is between 30 and 100 cm, and there is no uniform fashion for gastric bypass. The jejunum is transected with a white or camel cartridge linear stapler (Fig. 6.4), and the mesentery is divided with laparoscopic coagulating shears (LCS) including Harmonic Scalpel and SonoSurg (Fig. 6.5). Typically, the length of the Roux limb can be up to 200 cm without an associated increased incidence of malabsorptive complications. Jejunojejunostomy is performed with a side-to-side linear anastomosis using a white or camel cartridge linear stapler (Fig. 6.6), and the enterotomy is closed with a single layer of absorbable suture (Fig. 6.7). Some surgeons prefer to use a linear stapler to close the enterotomy, but this may cause stenosis. The mesenteric defect must be closed with a continuous, nonabsorbable suture to limit the possibility of an internal hernia (Fig. 6.8).



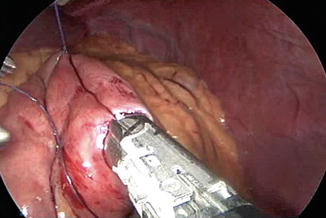
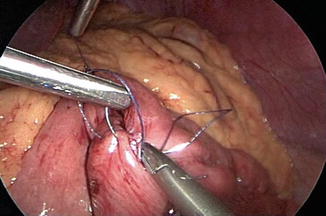
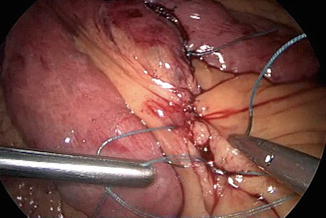
Fig. 6.3
Exposition of the ligament of Treits
Fig. 6.4
Transection of jejunum
Fig. 6.5
Division of the mesentery
Fig. 6.6
Jejunojejunostomy
Fig. 6.7
Closure of the entry hole
Fig. 6.8
Closure of the mesenteric defect
The Roux limb is passed in front of the transverse colon as is done in the “antecolic approach.” To reduce the tension to the gastrojejunal anastomosis, the omentum should be divided with LCS (Fig. 6.9).