This article will provide a thorough review of female genital anatomy relevant to labiaplasty and clitoral hood surgery. The anatomic variation in female genital anatomy makes tailoring the procedure to the individual patient a critical component of a successful surgery and esthetic outcome. Curvilinear trim resection is the most popular labia minora reduction technique. The alternative is the wedge. Clitoral hood reduction is rarely performed as a stand-alone procedure and is an adjunct to labiaplasty surgery, no matter the technique used. Labiaplasty has a high satisfaction rate and low complication rate.
Key points
- •
Labiaplasty surgery has become a commonly performed procedure in the United States due to increased awareness and the evolution of esthetic ideals.
- •
Understanding the anatomy of the female genitalia and the variations is a key to planning the appropriate surgical plan for achieving an esthetic outcome in labiaplasty surgery.
- •
Labiaplasty is performed with a curvilinear trim or wedge reduction, both acceptable and safe procedures with a low complication rate.
- •
Clitoral hood reduction is a balancing procedure commonly performed with labiaplasty and limited to skin excision.
- •
Postoperative care and instructions are essential in ensuring the patient’s timely and smooth recovery.
| ACOG | American College of Obstetricians and Gynecologists |
| HS2 | Herpes Simplex 2 |
Video content accompanies this article at http://www.advancesincosmeticsurgery.com .
Introduction: nature of the problem
An increasing number of women seek improvement regarding female genitalia, most often with concerns about the labia minora and clitoral hood. The American Society of Plastic Surgeons annual statistics report 10,592 labiaplasties performed in 2023, which has increased since it began reporting the procedure in 2015 [ , ]. The Aesthetic Society reported 18,120 labiaplasties in 2023, a 67% increase from the number reported in 2019 [ ].
The increase in awareness and demand for the procedure has been attributed to multiple factors: increasing awareness of a surgical solution, changing fashions that favor tight leggings and revealing clothes, contemporary pubic grooming, the representation of the vulva in mass media as hairless, flat, and with no protrusion beyond the labia majora, and the functional benefits of the procedure.
Historically, obstetrician-gynecologists have opposed the procedure. Genital esthetic surgery was condemned in the 2007 and 2019 American College of Obstetricians and Gynecologists (ACOG) Committee Opinion. ACOG published a formal article that vaginal rejuvenation and cosmetic vaginal procedures lacked data and efficacy to support these procedures [ ]. ACOG stated that procedure risks were too high and suggested reassurance to women for the wide variability of female genital appearance. As such, plastic surgeons tend to lead in publications and research and offer the procedure to patients.
There is no universal esthetic standard for the ideal vulvar complex and a vast presentation of varying anatomic variations. Additionally, the ideals and esthetics of female genital surgery continue to evolve with changing fashion, lifestyles, and social trends. Surgeons need to understand anatomy, ensure that our patients have realistic expectations of results, and choose the procedure that will create balance and harmony for the individual patient.
Anatomy and physiology
Understanding anatomy and anatomic variations can help optimize a tailored surgical approach. Normal labia minora anatomy encompasses a broad range of sizes, thicknesses, and colors.
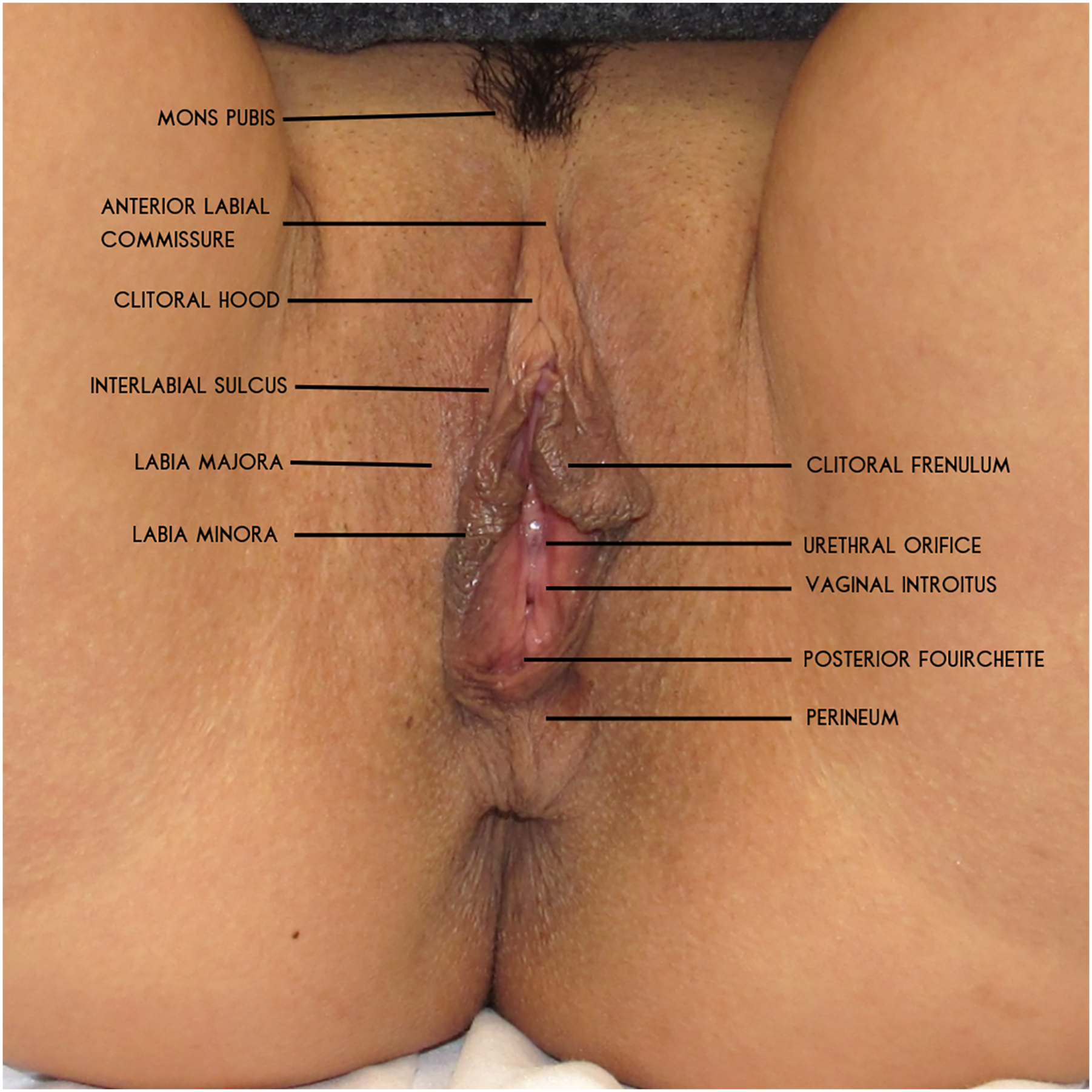
The basic anatomy of the external female genitalia has been well described. It consists of the mons pubis, the clitoris and its overlying clitoral hood, the labia minora, and the majora.
The focus of this text is primarily on the labia minora. The labia majora are 2 folds that extend posteriorly from the mons pubis (the triangular adipose tissue just anterior to the pubic symphysis) to the perineal area. The majora can be considered empty or redundant in some patients and addressed accordingly with volume restoration or reduction.
Enveloped and medial to the labia majora are the clitoris, clitoral hood, and labia minora. The minora and majora are separated by a sulcus.
The clitoris is positioned directly under the clitoral hood. The frenula are folds of skin of varying sizes that extend from the glans clitoris to merge with the extension of the clitoral hood to form the labia minora. There can be wide variations in the clitoral hood with the presence of lateral folds, heavy folds, small hoods, and variations in continuity with the labia minora.
The clitoral hood extends laterally and superiorly to the anterior labial commissure. The inferior border extended to the junction with the labial minora. This junction is the defining point of the frenulum, which is the portion of the labia minora that extends to the clitoris. The urethral meatus can usually be found at the frenulum’s apex.
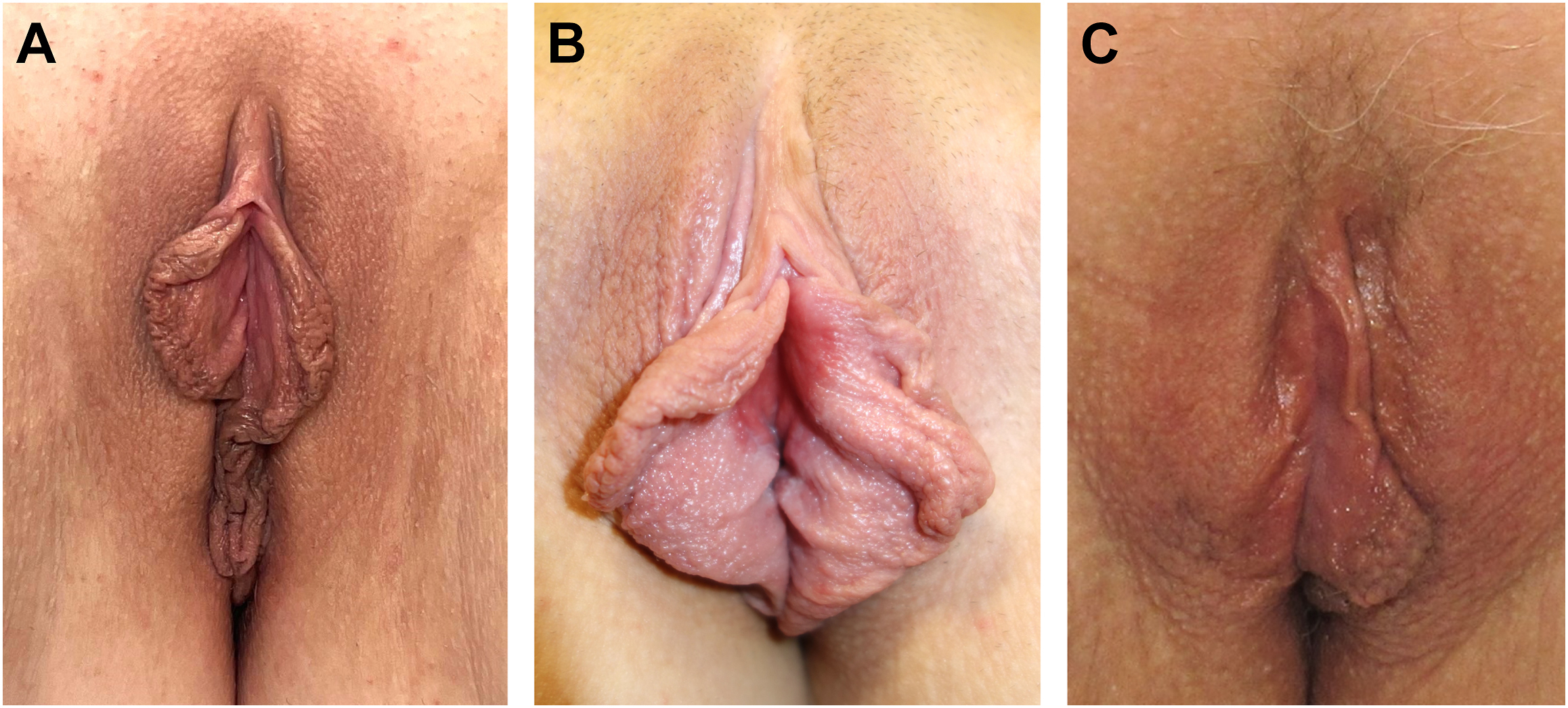
The labia minora continues posteriorly from the clitoral hood toward the perineal body. The labia can join posteriorly or remain separate and attach to the perineum. Variations in size, thickness, and pigmentation occur. The presence of rugae is common in those seeking labiaplasty ( Fig. 1 ).
The blood supply to the female genitalia consists of branches of the internal pudendal artery—the posterior labial artery and the perineal artery. This artery also gives rise to the dorsal artery of the clitoris. There are contributions from the external superficial pudendal artery via the anterior system. Georgiou and colleagues’s study determined the presence of a dominant central artery, which impacts the wedge technique’s healing and safety if not oriented properly [ ].
The innervation of the external female genitalia is through the pudendal nerve. The superficial branch becomes the posterior labial nerve, and the deep branch becomes the dorsal nerve of the clitoris. The dorsal clitoral nerve is deep to the clitoral fascia and the tunica albuginea. If the surgeon remains superficial to dartos fascia in this region, injury to clitoral innervation is unlikely.
There is no consensus as to how to classify the appearance of female genitalia. This is partly due to commonly referred aspects of the minora as hypertrophic or enlarged. However, studies have demonstrated that variation in the labial length, width, color, rugosity of the labial skin, and clitoral size encompasses a wide spectrum of normality. Several classification systems have been proposed, addressing the ability to measure or document the size and/or location of labial protrusion.
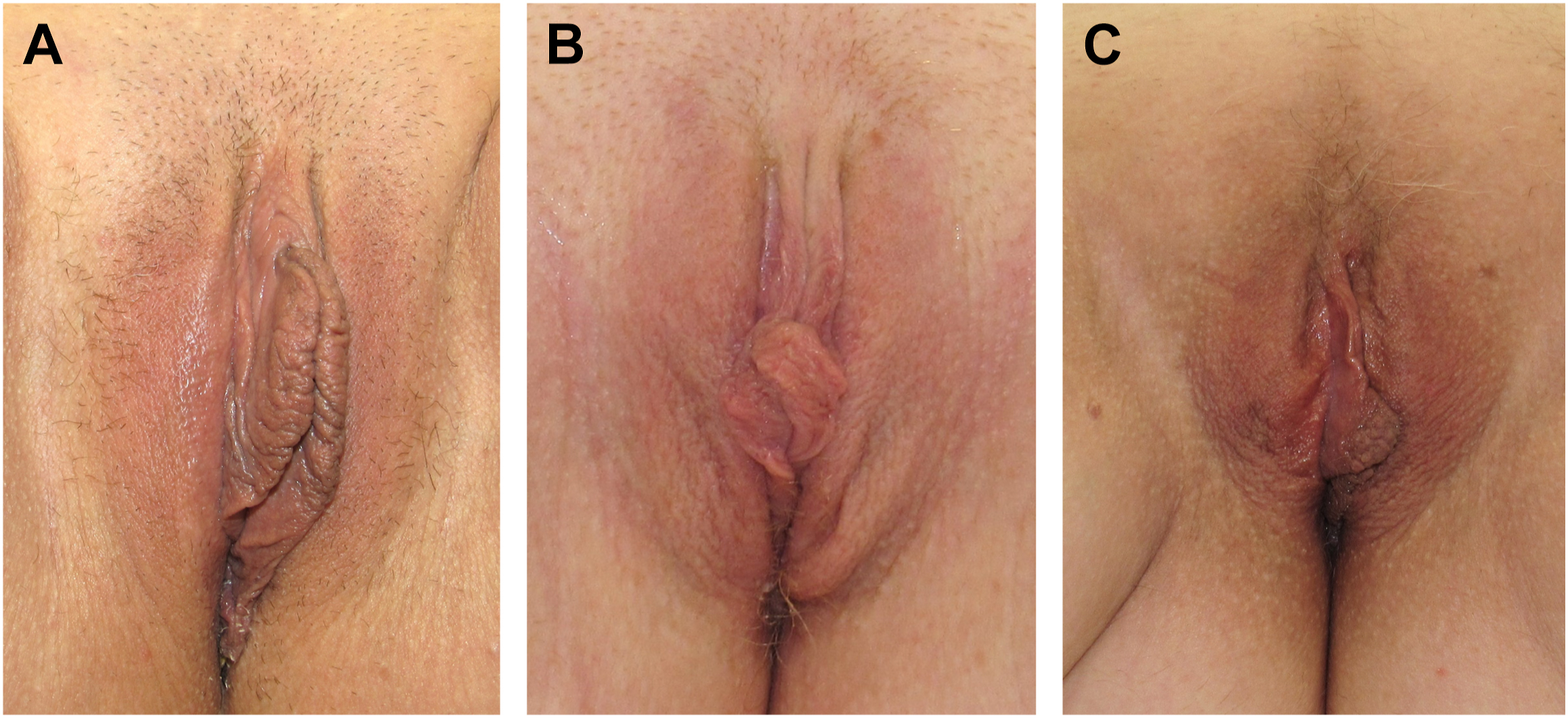
A commonly used classification system, the Banwell Classification system, serves as a clear means of documenting the labia anatomy, educating the patient, and informing the surgeon about the best labiaplasty technique [ ]. The Banwell Classification identifies the most prominent lateral point of the labia minora in either the upper, middle, or lower third of the vaginal vault. The thickness, rugosity, and pigmentation should also be noted. As with most bilateral anatomy, asymmetry is common and should be identified ( Fig. 2 ).
The posterior attachment of the labia minor also varies. The attachment may be low (close to the perineum), medium, or high. In some cases, there is a posterior connection or posterior fourchette ( Fig. 3 ).

The clitoral labial complex also encompasses a wide variety of anatomic variations. In most anatomic texts, the clitoral body and hood are small, but both can be enlarged. The clitoral hood can create a double fold with either horizontal or, more commonly, lateral fold excess. The junction between the clitoral hood and the labia minora is also varied ( Fig. 4 ).
Related posts:
 Combining Non-ablative Resurfacing with Radiofrequency Microneedling for Acne Scarring
Combining Non-ablative Resurfacing with Radiofrequency Microneedling for Acne Scarring
 Update on Anesthesia and Pain Management Strategies in Cosmetic Surgery
Update on Anesthesia and Pain Management Strategies in Cosmetic Surgery
 The Challenging Facelift
The Challenging Facelift
 Endpoints in Laser & Light-Based Devices
Endpoints in Laser & Light-Based Devices
 Social Media Dysmorphia
Social Media Dysmorphia
 Advances, Techniques, and Complications Associated with Adjacent Fat Transfer in Lower Blepharoplasty
Advances, Techniques, and Complications Associated with Adjacent Fat Transfer in Lower Blepharoplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


