While knee injuries account for just 7% of injuries in professional and collegiate baseball, they are the fourth most common cause of missed professional games. The 3 most common knee-related issues in baseball are patellar tendinopathy, meniscus tears, and medial collateral ligament sprains. While injuries such as anterior cruciate ligament tears and patellar dislocations are less common, they are notable due to their potentially significant effect on time missed. Treatment considerations of all these pathologies are multifactorial and should include skeletal maturity, level of play, timing of season/recruiting, and long-term goals.
Key points
- •
Knee injuries account for just 7% of injuries in professional and collegiate baseball, but those that require surgical intervention can lead to some of the longest amounts of absence from play among all musculoskeletal injuries.
- •
Patellofemoral injuries, meniscus tears, and medial collateral ligament injuries are the most common knee injuries in baseball, and each can be treated nonoperatively or with surgical intervention.
- •
Treatment considerations of all knee injuries in baseball are multifactorial and should include skeletal maturity, level of play, timing of season/recruiting, and long-term goals.
Introduction
The knee is one of the most commonly injured joints by athletes. Previous reports have indicated that up to 40% of sport-related injuries affect the knee joint, and that approximately half of knee injuries occur while playing sport. In baseball, knee injuries appear to account for a lower proportion of all musculoskeletal injuries; however, those that require surgical intervention can lead to some of the longest amounts of absence from play in Major League Baseball (MLB) and Minor League Baseball (MiLB).
Epidemiology
Recent reports have found that knee injuries represent just 6.5% of all MLB and MiLB injuries and 7% of all National Collegiate Athletic Association baseball injuries. While knee injuries may account for a low proportion of all baseball injuries, they can have a significant impact on time and games missed. In professional baseball, 12% of knee injuries require surgery, and knee injuries are the fifth most common cause of missed time and the fourth most common cause of missed MLB games.
While knee injuries can occur all around the baseball field, sliding appears to be a common mechanism of injury. In professional baseball, base runners are likely to experience noncontact injuries while sliding, and second base and home plate are common places for these sliding knee injuries to occur. , Knee injuries account for 12% of all sliding injuries in baseball and the knee is the second most commonly injured body part during feet-first slides.
The most common knee injuries that account for time missed in professional baseball are patellar tendinopathy, meniscus tears, and medial collateral ligament (MCL) sprains ( Table 1 ). However, in the senior author’s experience, some less common injuries, such as anterior cruciate ligament (ACL) ruptures and patellar dislocations, can have significant impacts on a player’s season or career. Thus, the goal of this study will be to provide an overview of the epidemiology and treatment options for each of these injuries when caring for a baseball athlete.
| Average Days Missed | % Requiring Surgery | % Season Ending | Most Affected Position | |
|---|---|---|---|---|
| Patellar tendinopathy | 11.8 | 5.4% | 8.9% | Pitcher |
| Medial meniscus tear | 111.2 | 54.5% | 24.1% | Catcher |
| Lateral meniscus tear | 118.9 | 54.1% | 31.1% | Pitcher |
| MCL sprain | 18.8 | 5.3% | 10.0% | Infielder |
Most common knee injuries in baseball
Patellofemoral Injuries
Patellar tendinopathy is the twenty-fifth most common injury in professional baseball, with an average of 11.8 days missed, 5.4% of cases requiring surgery, and 8.9% of cases being season ending.
Nonoperative treatment is preferred in cases of patellar tendinopathy, with surgical intervention reserved for athletes whose symptoms persist despite exhausting nonoperative options. , Nonoperative treatment may begin with eccentric strengthening, as a recent systematic review has concluded that eccentric strengthening is the only treatment of patellar tendinopathy supported by high-quality evidence. In addition, this early phase of treatment may include usage of a patellar tendon strap placed across the midportion of the tendon to reduce tensile stress. Patellar tendon straps have been shown to reduce pain, create more neutral knee alignment, and decrease landing forces during use ; thus, patellar strapping may be beneficial during training and alongside eccentric strengthening to slow progression of symptoms.
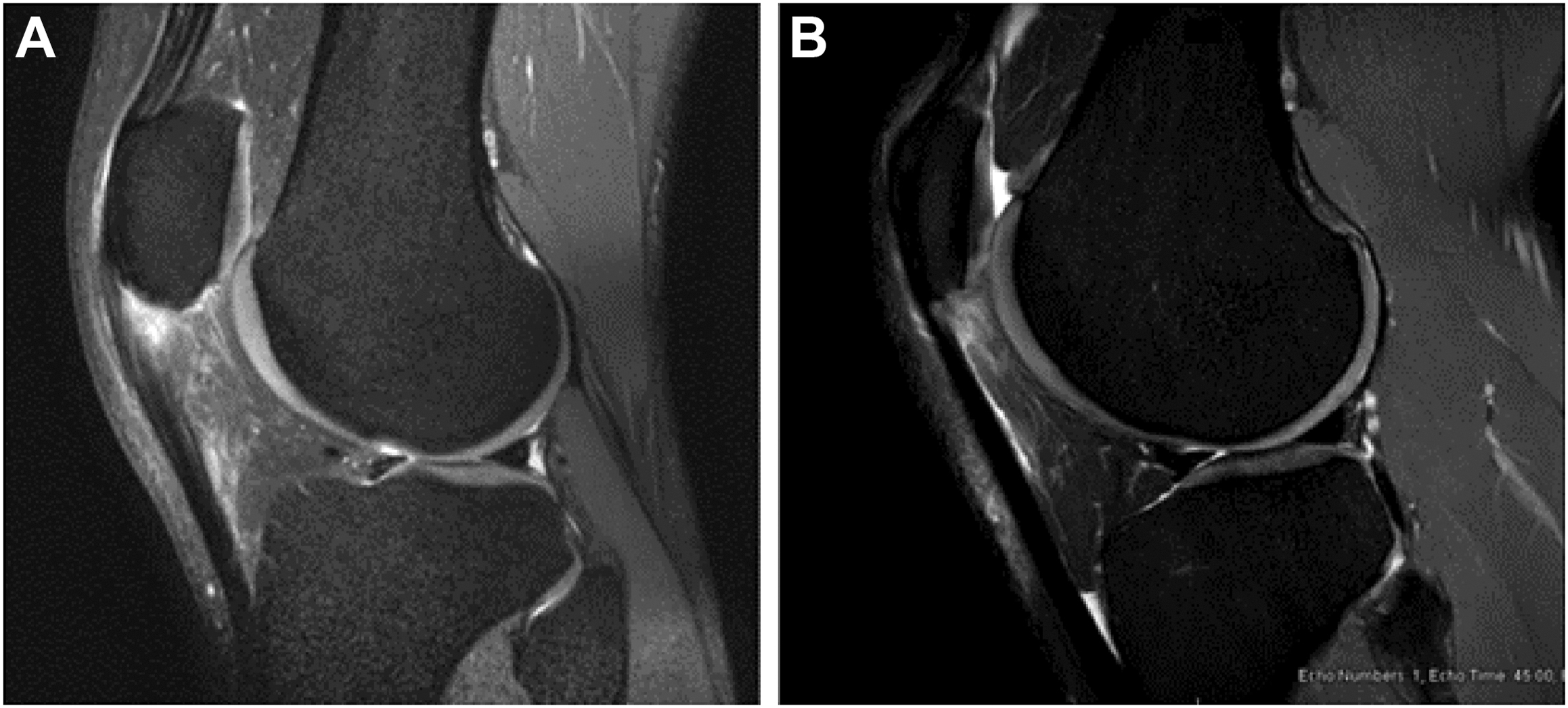
While corticosteroid injections are not recommended due to lack of evidence for their ability to provide long-term relief and the risk of tendon rupture that comes with steroid injections, platelet-rich plasma (PRP) and stem cell injections may be viable options in the treatment of patellar tendinopathy. PRP appears to be a safe treatment in recent systematic reviews, but more randomized controlled studies with long-term clinical outcomes are needed to determine its efficacy over other treatment options, , and it is not currently the personal choice of the senior author. There are similarly limited data on the efficacy of stem cell therapy for patellar tendinopathy, but some studies have reported statistically and clinically significant improvement in pain and function after ultrasound-guided injection of cell-based therapies. , The senior author’s preferred injection option for patellar tendinopathy is to use bone marrow mononuclear stem cells derived from the iliac crest rather than PRP or corticosteroid injections ( Fig. 1 ).
Athletes with chronic patellar tendinopathy whose symptoms are not well managed with nonoperative treatment may be indicated for surgical intervention, which may include patellar tendon debridement or repair. In a recent study reviewing outcomes after patellar tendon debridement in 37 athletes of various sports, 86.5% returned to play at an average of 3.5 months. However, in the senior author’s experience, return to play time may take 6 months or longer. In cases of patellar tendinopathy with extensive degenerative tissue at the insertion on the patella, patellar tendon rupture can occur, requiring surgical repair. In recent years, an increasing amount of evidence has supported the use of a bio-inductive collagen patch to augment healing potential during surgical repair, particularly in the context of midsubstance patellar tendon ruptures. , In a study of 18 MLB players who underwent patellar tendon repair, 100% of players returned to sport at an average of 182 days after surgery, which was significantly shorter than professional basketball, football, or soccer players. Notably, there was also no significant change in postoperative performance or number of games played.
Also common in patellofemoral pathologies among baseball players is patellofemoral chondrosis. Nonoperative treatment options are similar to those beneficial for patellar tendinopathy and include eccentric strengthening, bracing, and injections. In baseball, patellofemoral chondrosis is most common in catchers. As this is likely due to the increased forces on the patellofemoral joint during deep knee flexion, catchers with patellofemoral pain can wear knee savers to prevent deep flexion and protect the joint. In cases of small focal defects, arthroscopic debridement may be effective, with osteochondral allograft transplantation considered for larger defects (>1 cm) along with potential tibial tubercle osteotomy to offload the joint space.
Meniscus Injuries
Medial and lateral meniscus injuries combine to be the thirtieth most common injury in baseball and have the second and third highest rates of surgery respectively among professional baseball injuries. With over half of meniscus injuries in the MLB and MiLB requiring surgery, 24.1% of medial meniscus tears are season ending and 31.1% of lateral meniscus tears are season ending. While the number of meniscus injuries has decreased over time, the rate of surgery has increased, potentially due to the increased understanding of the importance of the meniscus for long-term joint preservation. MLB players are more likely than MiLB players to both return to sport and return to sport at the same level, and overall, catchers have the lowest return to sport rate of all positions.
Nonoperative treatment is not common for acute meniscus injuries, but degenerative tears may be treated without surgical intervention, especially when players are in season. Conservative treatment may include quadriceps strengthening or bracing to unload the affected compartment.
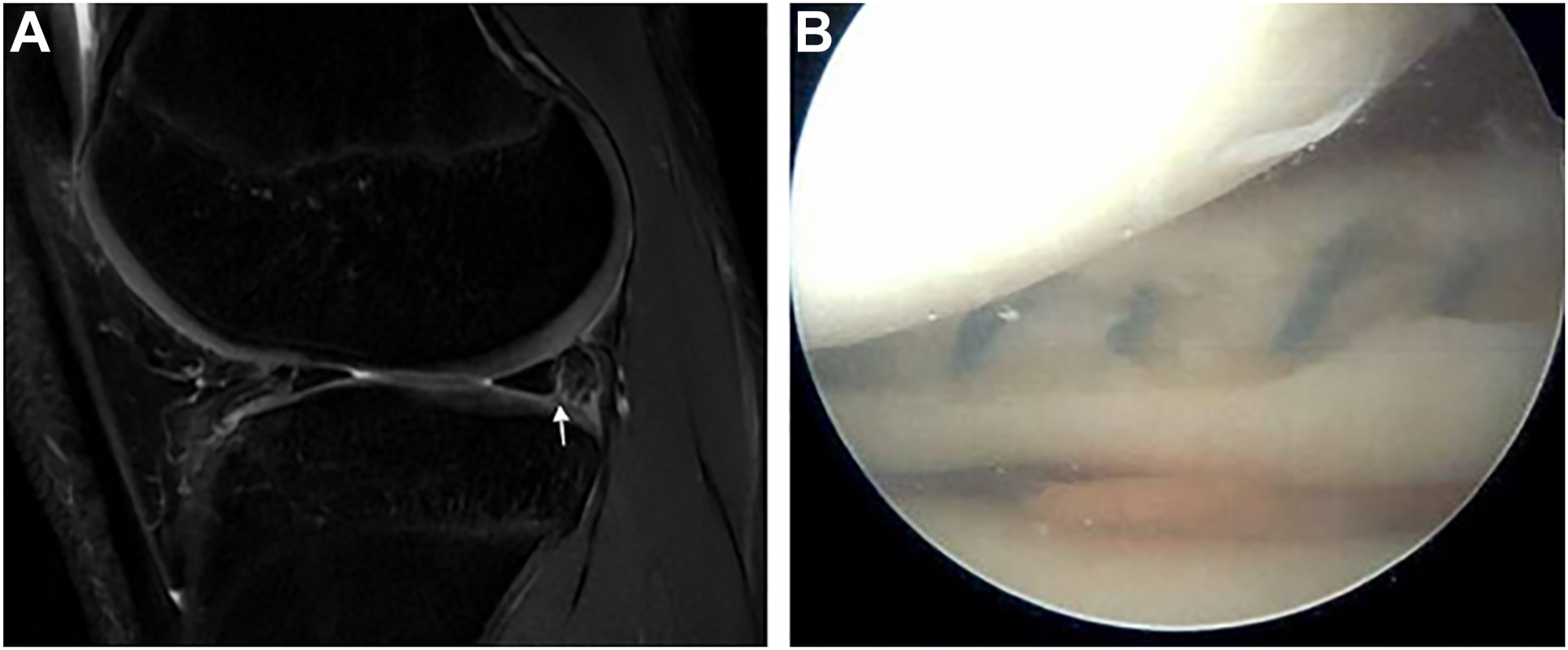
Surgical intervention may include repair ( Fig. 2 ) or meniscectomy. In professional baseball players, lateral meniscus repairs account for 72% of all meniscus repairs. This follows recent recommendations for elite athletes, as it is theorized that the lateral meniscus has better healing potential than the medial meniscus. In the MLB, 74% of players who underwent meniscus repair between 2010 and 2017 returned to sport at an average of 209 days, with 68% returning at the same or higher level of play. There has been no reported difference in return to play rates between lateral and medial meniscus repairs. In this time frame, 19% of MLB players who underwent meniscus repair experienced a second meniscus injury and underwent subsequent meniscectomy within 2 years of their initial repair. Of these players, all but one was able to return to the same level of performance after their subsequent meniscectomy.
Overall, 80% of MLB players who underwent meniscectomy from 2010 to 2017 returned to play at average of 42 days, with 76% returning at the same or higher level of play. Notably, 47% of these players were able to return during the same season. The difference in time to return to play is perhaps the most important consideration when deciding between meniscus repair and meniscectomy for a professional baseball player. Due to the importance of the meniscus in protecting the articular cartilage, repair is preferable for long-term knee health, especially for large tears. Large reparable tears should be repaired acutely, but smaller tears can sometimes be repaired after the season ends, or partial meniscectomy can be performed in season with relatively quick return to play.
Other surgical treatment options for meniscus tears have not been extensively researched, potentially due to a lack of cases in professional baseball. One retrospective case series investigating meniscal allograft transplantation (MAT) in professional athletes included 1 MLB player who underwent MAT that had to be subsequently repaired 1 year later. Overall, 77% of the athletes included in this study, including the MLB player, returned to play at the same level.
Medial Collateral Ligament Injuries
MCL injuries are the thirty-sixth most common injury in professional baseball, with an average 18.8 days missed, 5.3% of cases requiring surgery, and 10% of cases being season ending.
Nonoperative treatment is preferred for grade I or II proximal MCL tears and can include bracing to prevent valgus overload along with physical therapy to work on range of motion. It is possible for these athletes to return to play within 1 to 2 weeks of their injury. For low-grade distal tears, the same bracing and physical therapy protocols may be followed, but on a slower timeline to prevent further stress to the MCL, as previous reports have showed decreased healing potential for distal MCL injuries. , These athletes may return to play 3 to 4 weeks after their injury when they exhibit full range of motion with limited pain and instability.
Grade III MCL injuries may be treated surgically. While the surgical treatment of isolated, primary MCL tears is controversial, there are cases in which there is general agreement that surgical intervention is necessary. In cases of a complete avulsion off its proximal attachment, the medial patellofemoral ligament may also avulse off the medial epicondyle, thereby requiring repair of both ligaments. Additionally, distal MCL ruptures with a Stener-like lesion are less likely to heal nonoperatively and typically require surgical repair. In these cases, athletes may return to play around 6 months after surgery.
Other injuries of note
Anterior Cruciate Ligament Injuries
ACL ruptures only account for 2% of knee injuries in professional baseball, but they result in the highest amount of absence from play, with 156.2 days missed on average. Overall, 88% of MLB players who undergo ACL reconstruction (ACLR) return to play, but these players average 21.1% fewer career games than their teammates and batting average was significantly decreased in players who underwent ACLR on their rear batting leg. This significant impact on playing time and performance has led to ACL tears in baseball being studied more than some other knee injuries despite its relative infrequency.
Nonoperative treatment after ACL rupture is not recommended for professional athletes due to the risk of recurrent instability and secondary meniscus and cartilage injury that comes with delayed surgery. In terms of graft choice, there have been no studies at this point examining graft choice in a cohort of baseball players. However, among young active patients overall, allograft is not recommended, as evidence has shown allograft usage in these patients is a risk factor for retear and these patients report significantly lower activity levels than their autograft-receiving counterparts 2 years after surgery. Between autograft options, bone-patellar tendon-bone (BPTB) autograft is recommended over hamstring tendon autograft due to evidence showing higher retear rates in young athletes who undergo ACLR with hamstring tendon autograft. This seems to follow trends in professional and collegiate American football, with 86.1% of surgeons choosing BPTB autograft for their football athletes. However, if hamstring tendon autograft is to be used, addition of a concomitant lateral extra-articular tenodesis has been shown to reduce retear rates and rates of persistent rotatory laxity. For baseball athletes, the senior author prefers BPTB autograft but considers quadriceps tendon autograft if the athlete has a history of anterior knee pain or Osgood–Schlatter disease.
Patellar Dislocations
Patellar dislocations are extremely uncommon in baseball, but they are possible in many of the twisting noncontact movements that occur in baseball, and there have been a few instances of patellar dislocations in MLB players in recent years. While there has been no research on time missed after patellar dislocation in baseball, surgical stabilization is often recommended due to the high recurrence rate after primary patellar dislocation, meaning athletes may not return to sport for 6 or more months after surgery.
Anatomic and demographic risk factors should be taken into consideration when deciding whether to treat first-time patellar dislocations acutely or postpone surgery to the offseason. The senior author finds several prediction models and scoring systems to be helpful when counseling athletes on this decision. First, a prediction model has been developed to recommend treatment based on the 4 recurrence risk factors with the highest odds ratios ( Table 2 ). These include trochlear dysplasia, history of contralateral dislocation, skeletal immaturity, and Caton-Deschamps index greater than 1.45. Second, the patellar instability severity score can be used to determine which patients may be at higher risk of recurrence based on 6 risk factors ( Table 3 ). Athletes who are at lower risk of recurrence based on these models may succeed with conservative treatment or can postpone surgery to the offseason, whereas those who are at higher risk may require acute surgical stabilization with concomitant osteotomy to realign the joint.
Related posts:
 In Season Return to Play Issues for the Baseball Player
In Season Return to Play Issues for the Baseball Player
 The Physical Examination of the Throwing Elbow
The Physical Examination of the Throwing Elbow
 The Physical Examination of the Throwing Shoulder
The Physical Examination of the Throwing Shoulder
 Core and Lower Extremity Muscle Strains in Baseball Players
Core and Lower Extremity Muscle Strains in Baseball Players
 Rehabilitation of the Shoulder and Elbow in the Throwing Athlete
Rehabilitation of the Shoulder and Elbow in the Throwing Athlete
 Foot and Ankle Injuries in Baseball
Foot and Ankle Injuries in Baseball
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


