Keystone Flaps
Theodore A. Kung
Peter Neligan
DEFINITION
The keystone flap is a versatile fasciocutaneous flap that transfers available soft tissue to an adjacent defect and can be designed anywhere on the body where perforators are present. It serves as a reliable alternative to more complex forms of reconstruction, such as free tissue transfer, and can be used for large as well as small defects.
Advantages of keystone flaps include simple and rapid dissection that results in relatively shorter operative times compared to alternative reconstructive options, techniques that are easily reproducible and teachable, and reconstruction with local tissue of similar quality. In addition, although keystone flaps are based on perforating vessels, there is no need to perform a meticulous perforator dissection.
Appropriate use of a keystone flap over other choices of reconstruction (eg, muscle flap with skin graft, myocutaneous flap, free flap) can minimize donor-site morbidity and facilitate a more expeditious postsurgical recovery.
ANATOMY
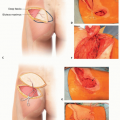
The keystone flap is a fasciocutaneous advancement flap. The donor-site secondary defect is addressed by performing two V-Y closures.
Knowledge of the location of musculocutaneous and septocutaneous perforators can facilitate design of well-vascularized keystone flaps (FIG 1).
Anteriorly, perforators from the internal mammary, intercostal, and epigastric systems can supply keystone flaps for chest and abdominal reconstruction.
Posteriorly, midline closures may take advantage of paravertebral intercostal perforators. Multiple perforators arising from the subscapular system may be used to design keystone flaps for the mid and upper back. Lower back and buttock keystone flaps can include perforators from the posterior intercostal, lumbar, and gluteal systems.
In upper and lower extremities, numerous perforators from the major longitudinal vessels can supply keystone flaps of various sizes. For larger defects, named perforators can be used to ensure adequate vascularity to the flap (eg, perforators from the descending branch of the lateral circumflex femoral artery), whereas smaller defects may depend on randomly distributed perforating vessels emanating from the underlying fascia and muscle.
One notable location where keystone flaps may fail is the scalp due to its axial blood supply and relatively unyielding quality.
In principle, to close a defect with a keystone flap, the volume of the keystone flap needs to be redistributed in order to fill nearly all of the primary and the secondary defect (the total defect size, primary plus secondary, is modestly reduced during closure due to advancement of the wound margins). Thus, the keystone flap is not an ideal choice to fill large concave defects. In those instances, one should consider reconstructive options that provide additional tissue volume.
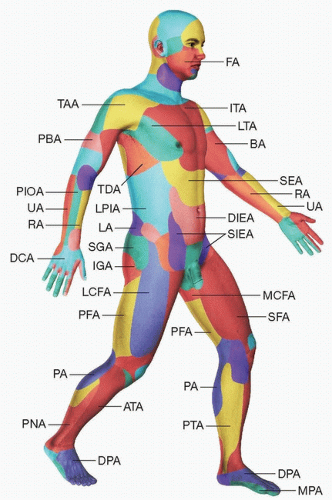
FIG 1 • Keystone flaps may be designed based on knowledge of the location of major perforators and their vascular territories. ATA, anterior tibial artery; BA, brachial artery; DCA, dorsal carpal arch; DIEA, deep inferior epigastric artery; DPA, dorsalis pedis artery; FA, facial artery; IGA, inferior gluteal artery; ITA, internal thoracic (mammary) artery; LA, lumbar arteries; LPIA, lateral branches of posterior intercostal arteries; LTA, lateral thoracic artery; MCFA, medial circumflex femoral artery; MPA, medial plantar artery; PA, popliteal artery; PBA, profunda brachial artery; PFA, profunda femoris artery; PIOA, posterior interosseous artery; PNA, peroneal artery; PTA, posterior tibial artery; RA, radial artery; SEA, superior epigastric artery; SFA, superficial femoral artery; SGA, superior gluteal artery; SIEA, superficial inferior epigastric artery; TAA, thoracoacromial artery; TDA, thoracodorsal artery; UA, ulnar artery.
More than one keystone flap can be designed around a defect in order to distribute the tension burden of secondary defect closure.
HISTORY
As described by Behan in 2003, the keystone flap is a trapezoidal perforator advancement flap. The name is derived from the flap’s resemblance to the shape of an architectural keystone within an ancient Roman arch.1
The keystone flap has been successfully applied to a vast array of clinical scenarios, including reconstruction of the trunk, head and neck, extremities, and perineum.2,3,4,5,6,7
PATIENT HISTORY AND PHYSICAL FINDINGS
The potential use of a keystone flap can be noted preoperatively during physical examination. Patients should be counseled that flap selection is ultimately based upon the dimensions of the defect as well as the laxity of the surrounding tissues. Therefore, other possible reconstructive options should also be reviewed with the patient before surgery.
For reconstruction after tumor extirpation, knowledge of the necessary surgical margins is helpful to predict if adequate local tissue will be available for design of a keystone flap. Extensive surgical margins commonly result in a wide concave defect that demands a significant amount of volume replacement. On these occasions, the keystone flap may not provide sufficient volume for coverage.
The need for preoperative or postoperative radiation therapy should be noted. A keystone flap using soft tissues that have been previously radiated can demonstrate significantly decreased laxity and may not adequately advance into the defect. When postoperative radiotherapy is planned, the well-vascularized keystone flap can be expected to sustain radiation without major complications.
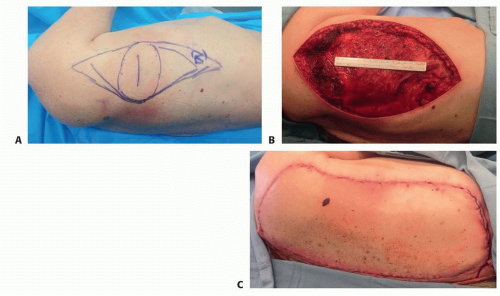 FIG 2 • A-C. Wide excision of a sarcoma of the lateral back. A large keystone flap was used to advance skin and soft tissue from a posterior to lateral direction. Adequate exposure is critical to designing a keystone flap of sufficient size to fill such a large defect. |
IMAGING
Imaging studies are not required for successful design of a keystone flap, but oftentimes, preoperative CT scans obtained for surgical planning are helpful to identify perforators.
Use of a handheld pencil Doppler probe can assist in identifying perforators to help design the keystone flap. Smaller keystone flaps supplied by random perforating vessels may not demonstrate Doppler signals but can still be used successfully.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree