Summary
Nasal reconstruction is the most technically challenging facial reconstruction.
There are special considerations to be made when reconstructing defects in the upper two-thirds versus the lower third of the nose.
The difficulty in reconstructing the lower third lies in consistency in intersecting anatomic concavities and convexities and the relative immobility of its skin.
Three distinct reconstruction considerations must be made: lining, support, and coverage.
Poor choices and execution can result in irreversible deformities.
12.1 General Principles of Nasal Reconstruction
The nose is the most prominent feature of the face with complex curvatures and contours. The intersecting concavities and convexities are distinct. Additionally, the overlying skin of the nose varies in thickness and composition with the upper two-thirds being thin and the lower third being thick and sebaceous. 1 These external characteristics as well as tremendous functional requirements make reconstruction of the nose a significant operative challenge. Currently, the overwhelming majority of nasal soft-tissue defects result from nonmelanoma skin cancer excision. The presence of the nose as the most prominent feature on the face lends it most susceptible to sun exposure with resulting ultraviolet damage and subsequent skin cancer. 2 Currently, the nose is the most common site of skin cancer of the head and neck with nearly a quarter million new cases of nasal nonmelanoma skin cancers diagnosed every year. The current standard of care for skin cancers on the nose involves Mohs histographic tumor excision and reconstruction by a surgeon. The obvious immediate advantages of a Mohs excision are a very low recurrence rate and preservation of the maximum amount of native tissue. 3 As opposed to other areas of the face, successful nasal reconstruction requires reconstructive requirements that include unique coverage lining and framework. Dr. Burget and Menick, the current champions of nasal reconstruction, spent a lifetime dedicated to finessing nasal reconstruction and several points inherent to their practice are essential concepts for any surgeon interested in nasal reconstruction. The most important, and at times the most confusing, is the concept of subunit versus defect reconstruction. Understand that the nose has nine nasal subunits and these are based on transitions in the shadows between natural convexities and concavities of the nose. 4 The arguments for either re-creating a partial subunit defect or reconstruction of the entire subunit are based both on the actual technical execution and the final result. The lower third subunits include the alar lobule, soft triangle, the paired soft triangles, and the single tip. 4 The conversion of partial defects of the subunit that comprises 50% or less into total subunit defects will result in the surgeon’s incisions along natural crease lines, as well as the valid argument that a practitioner who repairs an entire ala or tip subunit repeatedly becomes adept at re-creation of the entire subunit every time. Simplicity, repeatability, execution, and improved final aesthetic results are expected from the practice of subunit reconstruction. The arguments against subunit reconstruction are varied and argue against resection of “normal tissue” with the resultant requirement of larger donor sites with subsequent morbidity. 5 It is also important to understand that subunit reconstruction has never been advocated for the upper two-thirds of the nose, that is, the dorsum or sidewalls. Remember that these areas are fairly flat and featureless. There is no inherent advantage to placing scars within the borders of these areas and in fact the majority of these defects can be repaired with full-thickness, defect-only skin grafting. It is prudent to be aware and adept at subunit and defect reconstruction, and be able to practice both. Blind dogmatic approach of either technique without fully understanding the principles and basis behind it is poor surgical practice and will ultimately yield inferior final results versus accurate individual assessment and appropriate technique application. Additionally, the beginning practitioner can often be overwhelmed by the literally hundreds of descriptions of various surgical techniques for nasal reconstruction often involving geometric local flaps. Understand that the current masters of nasal reconstruction use collectively less than half a dozen surgical techniques and are able to demonstrate results that are essentially a normal anatomic reconstruction with very minimal donor-site morbidity. The lesson here is that a practitioner would be well served to truly understand the most basic techniques of nasal reconstruction and finesse a few individual techniques versus a partial familiarity with a large number of techniques. In fact, the overwhelming majority of nasal defects can be managed with either full-thickness grafting or the paramidline forehead flap.
12.1.1 Regional Considerations: Upper Two-Thirds versus Lower One-Third of the Nose
Reconstruction of isolated defects of the upper two-thirds of the nose is straightforward. The region is relatively featureless and the skin is thinner and can be lax in elderly patients and often simple techniques can be applied. Initially, primary closure either vertically, taking advantage of the cheek laxity, or horizontally, taking advantage of nasal tip descent, can be performed. Larger defects without exposed cartilage can be managed with color-matched full-thickness skin graft. A full-thickness skin graft can be used for defect-only reconstruction without regard to subunits, given there is no inherent advantage demonstrated in a formal subunit reconstruction, placing these scars on the upper two-thirds. With regard to local flap closure, bilobed flaps offer no improved aesthetic advantage over careful linear closure on upper two-thirds of defects. A well-designed banner flap can recruit lax cheek skin providing ideal scar placement. For thicker sidewall defects, a V-Y advancement flap with a vertical limb placement on the cheek–nose junction is useful. The circumstances of combined cheek nasal defects with exposed nasal cartilage or bone are common and can be well managed by simultaneous cheek advancement flap with subcutaneous turnover flap to provide nasal bone and cartilage coverage with subsequent full-thickness grafting.
Finally, larger defects of the nasal dorsum or sidewall with exposed bone or cartilage or significant potential contour deformity can be managed with forehead flaps.
Lower third nasal reconstruction is considerably more difficult than upper two-thirds nasal reconstruction. Skin is thicker, sebaceous, and less mobile. The region is dominated by intersecting anatomic convexities and concavities. Additionally, the ala does not tolerate retraction of the alar rim. Alar retraction and asymmetry are common with poor local flap design and remarkably difficult to correct. For these reasons, very accurate planning, reconstructive method selection, and execution are required. Poorly executed full-thickness skin grafts, although simple in nature, can result in unmistakable long-term deformities.
Additionally, the single-staged melolabial flap is useful for small (1.2 cm or less) posterior ala defects. 6 This is simply a transposition flap taking advantage of the cheek laxity with a planned dog-ear excision. The cheek skin is transposed, the dog-ear is excised, and then the flap is inset with great care to reapproximate the cheek–nose junction. Understanding that the flap disrupts the cheek–nose junction and diminishes the normal alar curve, and often requires a secondary revision procedure.
12.2 General Techniques for Closure of Simple Nasal Defects
Allowing the defect to heal by secondary intention or heal with assisted wound-healing agents.
Color-matched full-thickness skin grafting.
The rearrangement of nasal skin by the use of local flaps.
12.2.1 Secondary Healing
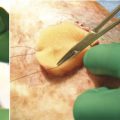
The first category, secondary healing or healing by assisted wound healing agents usually an extracellular matrix (ECM) has a limited but expanding utility in nasal reconstruction. Although there is increasing reliance of wound healing agents to allow the body to heal in secondarily without surgical repair, often resulting in equivalent or superior aesthetic results, the usefulness of these agents for nasal reconstruction is currently limited. The requirements for a functional reconstruction with accurate airway flow patterns and the aesthetic intolerance of alar retraction do not permit a wide range of secondary healing. Secondary healing does work well for medial canthal and nasal sidewall defects where the deep buttress bone prevents late contraction; however, on the thickened skin of the lower third and in particular large nasal sidewall defects, more superior aesthetic results can currently almost always be reached with surgical repair (▶ Fig. 12.1).

Fig. 12.1 Defect directly after Mohs excision shown, with results shown at 3 weeks and 2 months.
12.2.2 Full-Thickness Skin Grafting
The second general technique is full-thickness skin grafting. It is useful to break down the nose into upper two-thirds and lower third anatomic regions. Invariably, the upper third can be treated by non-subunit, that is, defect-only full-thickness grafting, for the vast majority of defects. 7 Understand that the full-thickness grafts need to be harvested from a supraclavicular location for final color match. Our selection of donor site is based almost entirely on the size of the defect, as well as the thickness of the defect. The smaller defects can be managed with forehead, preauricular or postauricular donor sites, whereas larger defects require full-thickness grafting from supraclavicular neck incisions. 8, 9 The exception to full-thickness grafting for upper two-thirds defects is only with exposed cartilage or defects of such thickness that a noticeable contour deformity will be incurred from simple full-thickness grafting. Additionally, a special category of a combined cheek and nasal defect with exposed nasal cartilage deserves special management. For full-thickness defects with exposed cartilage, the surgeon’s choice is to either allow it to heal in secondarily to allow granulation tissue to develop along the base, which can be successfully grafted, or inclusion of similar ECM to facilitate the incorporation of a soft-tissue bed that will support full-thickness grafting. Additionally, there are instances, particularly in young patients, that such large defects in the upper two-thirds require forehead flap reconstruction to adequately fill in or recreate soft-tissue contour defects, but these are relatively infrequent.
The use of full-thickness skin grafts on lower third defects has long been an issue in plastic surgery. Traditional plastic surgery teaching has often derided lower third skin grafting as an unacceptable operative choice with unacceptable final aesthetic results. This dogma perpetuated despite the dermatologist’s wide successful use of full-thickness grafting for lower third defects. In fact, with meticulous and disciplined approach to patient selection and graft selection, full-thickness grafting for lower third soft-tissue defects can yield superior aesthetic results. 10 Understand the characteristics of the lower third of the nose that is defined by the alar rims inferiorly, the nasolabial grooves laterally, and the alar groove, which forms a junction with the upper two-thirds of the nose, and is very intolerant of distortion of these margins. As discussed earlier, proper patient donor-site selection is essential to achieving optimal results. The criteria for selecting nasal defects that can be appropriately treated with full-thickness skin grafts include defect location and this would include 1.5 cm in diameter on the lower third, as well as the entire dorsum, the entire sidewall, with these defects remaining partial thickness with underlying dermis and subcutaneous tissue or perichondrium intact 10 (▶ Fig. 12.2).

Fig. 12.2 (a) New Mohs defect from basal cell carcinoma recurrence involving originally skin grafted repair. Foil pattern template and bolster sponge dimensions are created. (b) Final graft dimensions are transposed to neck donor site and the graft elevated and then thinned to the deep dermal layer. Note that graft is atraumatically handled throughout harvest by soon-to-be-discarded borders. (c) Graft is inset with continuous sutures of fast absorbing gut. Bolster sponge is coated with antibiotic ointment and sewn into place with 3–0 praline and 5–0 silk. (d) A 69-year-old female status post 2-cm Mohs excision for basal cell carcinoma at nasal tip. Defect-only reconstruction with color-matched full-thickness skin graft from supraclavicular donor site. Postoperative results shown at 1 month and again at 2 months.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


