Innervated Musculocutaneous Lip and Cheek Flaps
M. KARAPANDŽIć
EDITORIAL COMMENT
This is a classic description of one of the most important procedures currently used to reconstruct defects of the upper and lower lips. This is so particularly because of the attention paid to functional restoration of the oral sphincter.
The aim of reconstruction of lip defects by innervated musculocutaneous lip and cheek flaps is to form new lips that are anatomically and functionally able to satisfy the everyday needs of feeding, phonation, emotional expression, and communication. The reconstructed lip should be able to match the normal one, with parallel appearance, color, texture, hairiness, shape, thickness, elasticity, and dynamics of movement.
The reconstructive method of innervated musculocutaneous arterial flaps is based on the principle of replacing lost tissue with labial or cheek tissue that most closely resembles that of the lips. The flaps should contain skin, muscle, and mucous membrane with discrete blood and nerve supplies. This makes possible immediate mobility and normal sensibility with preservation of vegetative functions in a newly formed vermilion-bordered lip (1, 2, 3).
INDICATIONS
The procedure is applied in all patients in whom lip defects cannot be sutured directly without functional consequences. It is most frequently applied in defects caused by radical excision of malignant tumors and traumatic avulsion.
ANATOMY
Flaps are formed from all the anatomic elements of the lip and part of the cheek tissue. Essential elements of the flap are lip muscles covered with skin.
Lip muscles can be classified as either constrictors or dilators. The muscles are arranged in three layers: peripheral, medial, and deep. According to their position and function, these muscles may act as synergists or antagonists in the coordination of lip movement.
The orbicularis oris muscle is the most significant muscle. It is included in the structure of innervated musculocutaneous arterial flaps, together with the buccinator, both forming an orbicularis-buccinator complex that makes a newly formed lip equal in functional quality to the normal lip.
The orbicularis oris muscle is composed of several layers of muscle fibers that surround the lip orifice and stretch in various directions (Fig. 176.1). Its muscular structure may be divided into two concentric rings according to the origin of the fibers. The peripheral ring consists of muscle fibers that are radially located and inserted into upper and lower lips. The central ring consists of its own semicircular fibers that stretch obliquely through the thickness of the lip, running from the deep skin surface of one commissure toward the mucous membrane of the opposite commissure. The function of the centrally positioned orbicularis oris muscle is primarily sphincteric; the other lip muscles serve a supporting and dilatating function.
The facial artery with its branches, the inferior and superior labial arteries, supplies the innervated musculocutaneous flaps (Fig. 176.2). Adequate blood circulation in these flaps is extremely important, especially in elderly and previously irradiated patients. The anterior facial vein with its branches, the upper and lower labial veins, provides venous drainage. Lymphatic drainage is to the regional submental and submandibular glands.
The sensory innervation of the flaps originates from the second and third branches of the trigeminal nerve. Parts of the flap from the upper lip are innervated by the infraorbital nerve, and those formed from the remaining lower lip are innervated by branches of the mental nerve. The commissure area derives sensory innervation from the buccinator nerve.
The motor nerves that are preserved with the flap originate from the buccal and mandibular rami of the facial nerve. The superficial buccal branches pass under the skin and over the superficial facial muscles, which they innervate. Deep fibers supply the zygomatic and quadratus muscles of the upper lip; the deep buccal branches innervate the buccinator and orbicularis oris muscles. The ramus marginalis passes forward under the platysma and the triangularis, supplying innervation to the lower lip muscles and the chin (see Figs. 176.1 and 176.2).
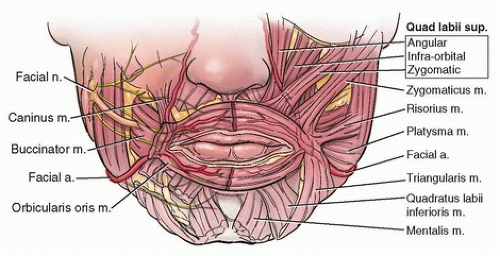 FIGURE 176.1 Anatomy of the lip muscles in layers and their participation in forming the peripheral ring of the orbicularis oris muscle. Position of the facial artery and its branches in relation to the muscles is shown. The branches of the facial nerve enter the orbicularis oris and the other lip muscles. |
FLAP DESIGN AND DIMENSIONS
The dimensions of innervated musculocutaneous arterial lip and cheek flaps depend on the size, position, and cause of the defect. Flaps can be located in the lower and upper lips in the area of lip angles or in both lips simultaneously. Defects are most frequently partial and rarely involve the whole lip. The most frequent defects are those of the lower lip, and they usually are located between the medial line and the commissure, rarely involving the central part.
Dimensions of defects that are suitable for lip reconstruction with this kind of flap are generally from 3 to 9 cm long. Flap width and length vary, depending on the pathologic process that caused the defect. Flaps are formed on both sides of the defect, and their width is equal to the height of the defect. The most suitable width of flaps is from 18 to 25 mm, and the flap should, in principle, have the dimensions of the orbicularis oris muscle.
Planning the flap begins with measurement of the lengths of the lower and upper lips and rima oris. The part of the lip to be excised is marked and measured. The defect is planned as a quadrilateral because this form is most convenient for the sliding and rotation of musculocutaneous flaps. From the edge of the planned defect, the width and length flap dimensions are marked on both sides and should follow the course of the orbicularis oris muscle and the natural lines of the face so that scars will not be noticeable.
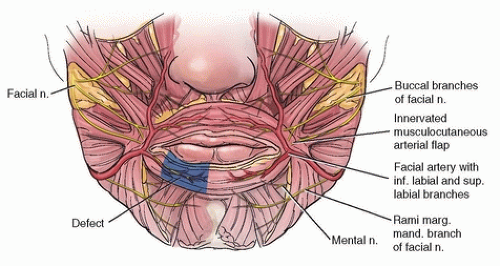 FIGURE 176.2 The separated orbicularis oris muscle with preserved motor and sensory nerves and the facial artery with its branches form the innervated musculocutaneous arterial lip and cheek flaps. |
The planned flaps should be long enough and wide enough that the newly formed lip may be constructed with an adequate rima oris for normal feeding, intelligible speech, and easy approach to the oral cavity for further therapeutic procedures. Adequate flap width allows encircling of the lip and prevents dribbling.
OPERATIVE TECHNIQUE
Defects of the Lower Lip
Full-thickness defects of the lower lip are reconstructed by the formation of two flaps from the remaining healthy lip tissue and tissue from the opposite lip, with the addition, in large defects, of some cheek tissue.
The operative procedure in forming innervated musculocutaneous arterial lip and cheek flaps is a continuous process in which nerve elements and blood vessels are sought simultaneously with selective cutting of some muscle fibers and separation of the orbicularis oris muscle into a special functional unit. From the edge of the defect, the incision advances at an equal distance from the mucocutaneous vermilion line, curving in the direction of the orbicularis oris muscle toward the lip commissure, which it curves around.
Then the incision continues at an equal distance over the nasolabial sulcus to the upper lip, to the area of the vertical
projection of the nasal wing. The flap is of equal width along its full length. The incision continues deep to the lip muscles toward the region of the commissure to the site where the surrounding muscles intermingle with the orbicularis oris muscle. To this point, the muscle fibers are gradually cut so that the incision reaches only the mucous membrane in the initial part of the flap. Then, with the preparation of surrounding supporting muscle, some muscle bundles are selectively cut and the orbicularis oris muscle is separated. In the region of the lip commissure, muscle fibers are cut only in the superficial layer, while the deeper fibers of the orbicularis and buccinator muscles are preserved. It is especially important to preserve the medial part of the buccinator muscle because these decussated fibers are contained in the composition of lower and upper lip muscles (see Fig. 176.2).
projection of the nasal wing. The flap is of equal width along its full length. The incision continues deep to the lip muscles toward the region of the commissure to the site where the surrounding muscles intermingle with the orbicularis oris muscle. To this point, the muscle fibers are gradually cut so that the incision reaches only the mucous membrane in the initial part of the flap. Then, with the preparation of surrounding supporting muscle, some muscle bundles are selectively cut and the orbicularis oris muscle is separated. In the region of the lip commissure, muscle fibers are cut only in the superficial layer, while the deeper fibers of the orbicularis and buccinator muscles are preserved. It is especially important to preserve the medial part of the buccinator muscle because these decussated fibers are contained in the composition of lower and upper lip muscles (see Fig. 176.2).
If the defect is not large, a smaller part of the triangularis muscle fibers (which continue toward the upper lip) and part of the caninus muscle fibers (which continue to the lower lip) can be preserved in the region of the commisure. Preservation of the triangularis and caninus muscle fibers is necessary so that the mobility of the musculocutaneous flap will not be damaged. In large defects, the orbicularis oris muscle is separated completely from the surrounding muscles; thus, the mobility of the flaps is increased. In all cases, buccinator muscle fibers are saved to maintain functional harmony of the facial muscles with the orbicularis oris muscle. In the upper lip region, only the superficial muscle layer is cut to separate the orbicularis oris muscle and to improve the mobility of the musculocutaneous flaps.
In flap preparation that selectively cuts muscle fibers to separate the orbicularis oris muscle, full attention must be given to preserving the motor and sensory nerves and the facial artery and all its branches. The whole surgical procedure is directed mainly toward finding and preserving the nerve elements and the vascular network. It is usually necessary to use magnifying loupes during preparation of the nerve elements.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


