The shape of the human face is composed of a skeletal bony framework that is covered by a soft tissue envelope. Overall, skeletal proportions are probably the most important component of facial attractiveness. Fritz E. Barton Jr., 2009
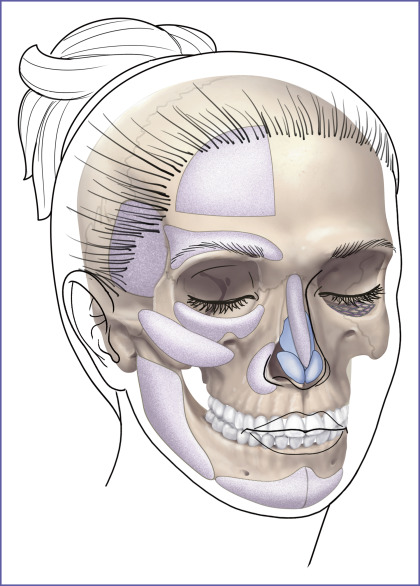
Since the skeletal infrastructure of the human face is fundamental to its appearance, its surgical change can be powerful. Conceptually, autogenous bone would be the best material to restore or augment the craniofacial skeleton because it has the potential to be vascularized and, then, incorporated into the facial skeleton. In time, it can be biologically indistinguishable from the adjacent native skeleton. Practically, the use of autogenous bone to augment facial skeletal contours is limited. Donor site morbidity as well as the time and operative costs associated with autogenous bone graft harvest can be significant. Furthermore, the inevitable resorption and the poor handling characteristics of autogenous bone grafts limit the quality and predictability of the aesthetic result. With the exception of interposition grafts used to reconstruct segmental load-bearing defects of the maxilla and mandible, the majority of craniofacial skeleton replacements and, particularly, facial skeleton augmentation is done with alloplastic implants. A diagrammatic survey of the alloplastic implants used for facial skeletal reconstruction and enhancement is presented in Fig. 1.1 . Subsequent chapters will address each anatomic area.
Patients with normal, deficient, and surgically altered or traumatically deformed anatomy may all benefit from implant augmentation of their craniofacial skeleton.
Facial Balance and Definition
Most often, facial skeletal augmentation is done to enhance facial appearance in patients whose skeletal relationships are considered within the normal range. They want more definition and angularity to their appearance. Other patients desire to “balance” their facial dimensions. The woman in Fig. 1.2 underwent chin and mandible angle augmentation at the time of rhytidectomy to provide angularity and balance between her upper and narrower lower face.

Skeletal deficiency
Craniofacial deformities that are disfiguring and are of functional consequence to vision, breathing, and mastication usually require skeletal osteotomies and rearrangement as treatment. Less severe midface and mandibular hypoplasia are common facial skeletal variants. In patients with these morphologies, occlusion is normal or has been compensated by orthodontics. These patients have neither respiratory nor ocular compromise. In skeletally deficient patients whose occlusion is normal or has been previously normalized by orthodontics, skeletal repositioning would necessitate additional orthodontic tooth movement. Such a treatment plan is time-consuming, costly, and potentially morbid. It is, therefore, appealing to few patients. In these patients, the appearance of skeletal osteotomies and rearrangements can be simulated through the use of facial implants. Diagrammatic representations of how implant surgery can mimic the appearance of skeletal osteotomies are shown in Figs. 1.3 and 1.4 .
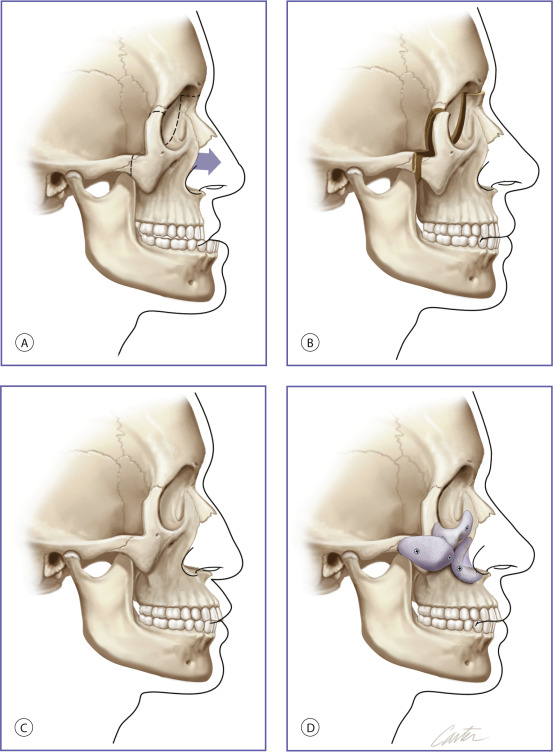
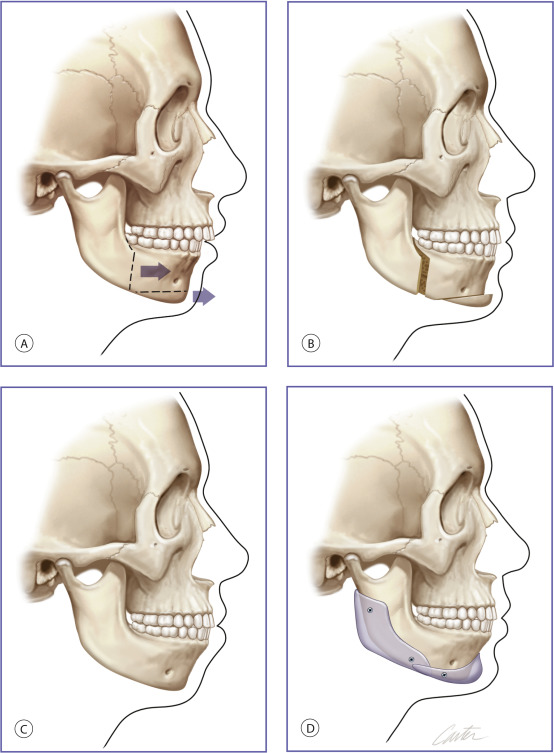
Fig. 1.5 shows a patient with corrected occlusion who underwent multiple implant correction of her midface and mandibular deficiencies.