div class=”ChapterContextInformation”>
16. Treatment in Children
Keywords
ChildrenHair lossAlopeciaAlopecia areataTrichotillomaniaTinea capitisAplasia cutisTrichorrhexis nodosaNethertonPili tortiMonilethrixTrichorrhexis invaginataTrichothiodystrophyUncombable hairWoolly hairGriseofulvinTerbinafineItraconazoleFluconazoleSteroidsMinoxidilIntroduction
Hair loss in children is a distressful situation for patients and, particularly, parents. Treatment of these patients is commonly a source of concern for physicians as well. It is important to correctly identify the cause of hair loss in children and to determine if there are any potential underlying medical conditions that will require further investigation and care. Additionally, lack of clinical trials and clinical research results in a paucity of data regarding treatment efficacy and safety in this specific population. Weighing the risks versus benefits of therapy for hair loss is a point that has to be readdressed in every consultation. In this chapter, we discuss treatment of common types of hair loss in children based on current literature and experience.
Patchy Alopecia
Tinea Capitis
Tinea capitis (TC) is an infection caused by dermatophyte fungal species of the genera Trichophyton and Microsporum [1–3]. It mainly affects children between 3 and 7 years of age [1].
Diagnosis
Clinical features: The presentation of tinea capitis may vary from asymptomatic alopecic patches with subtle scaling to inflammatory suppurative forms, depending on its cause and host immune factors (Fig. 16.1).
The gold standard is the identification of the species, by means of culture in Sabouraud agar. The material is obtained by scraping the scalp, using hairbrushes, toothbrushes, or cotton swabs [1, 3, 6].
The type of hair invasion may be observed on microscopy: endothrix is characterized by arthroconidia within the hair shaft, usually produced by Trichophyton spp. and ectothrix by the presence of hyphae and arthroconidia around the hair shaft, frequently associated with Mycrosporum spp. Endothrix favosa is most commonly caused by Trichophyton schoenleinii. In patients with tinea capitis favosa, infected hairs are characterized by the presence of hyphae and air bubbles within the hair shaft.
Trichoscopy: Features are very suggestive of the diagnosis of TC but do not point to the etiological agent. Characteristic features include comma hairs, corkscrew hairs, zigzag hairs, and Morse code-like hairs (Fig. 16.2) [2].
Wood’s lamp: green fluorescence in Microsporum infections and nonfluorescent in Trichophyton infections [3, 6].

Inflammatory tinea capitis with kerion formation in a girl
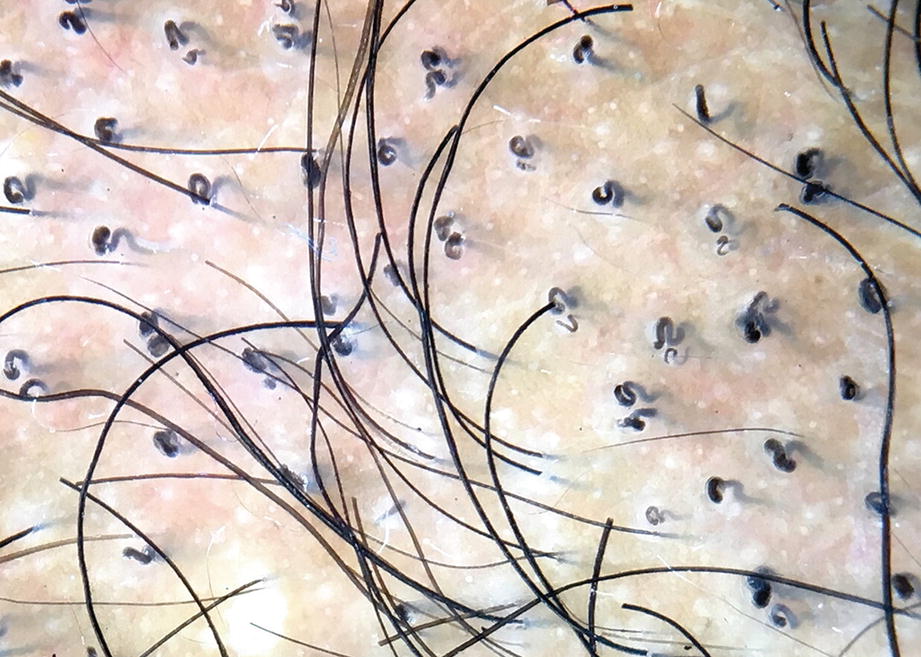
Trichoscopy using immersion fluid from a patient with tinea capitis showing typical comma and corkscrew hairs
Management
Oral treatment for tinea capitis
Drug | Structure | Dose | Duration | Formulation |
|---|---|---|---|---|
First-line treatment | ||||
Griseofulvina | Spiro-benzo [b]furan | Microsized: 20–25 mg/kg/day | 6–8 weeks | Tablets 500 mg Oral suspension 125 mg/5 mL |
Ultramicrosized:10–15 mg/kg/day | 6–8 weeks | Tablets 125 or 250 mg | ||
Terbinafineb | Allylamine | 4–6 mg/kg/day based on weight <25 kg: 125 mg 25–35 kg: 187.5 mg >35 kg: 250 mg | Trichophyton spp.: 2–6 weeks Microsporum spp.: 8–12 weeks [3] | Granules 125 mg or 187.5 mg Tablets 250 mg |
Second-line treatment | ||||
Itraconazolec | Triazole | 3–5 mg/kg/day | Trichophyton spp.: 2–4 weeks Microsporum spp.: 4–6 weeks [3] | Capsules 100 mg Tablets 200 mg Oral suspension 10 mg/mL |
Fluconazole | Triazole | 3–6 mg/kg/day | 3–6 weeks | Tablets 50, 100, 150, 200 mg Oral suspension 50 mg/5 mL or 200 mg/5 mL |
Additional treatments (used only in association with systemic antifungal therapy) | ||||
Topical agents: Ketoconazole 2%, selenium sulfide 1% or 2.5%, and ciclopirox olamine 1% or 1.5% shampoo 2–3 times per week for at least 4 weeks | ||||
Steroids: To be considered in inflammatory cases. Use is controversial. Suggested dosage: Prednisolone 0.5 mg/kg/day (short course ~2 weeks) | ||||
Griseofulvin and terbinafine are the only drugs approved by the Food and Drug Administration (FDA) for the treatment of TC in children. Terbinafine is more effective against the Trichophyton spp. and griseofulvin against Microsporum spp. [1, 3, 4, 6] Itraconazole is considered a second line of treatment. It seems to be safe, well tolerated, and effective in continuous or pulse regimen against both Microsporum [8–10] and Trichophyton species [6, 8, 9]. For refractory cases, fluconazole is a therapeutic option [6, 11].
Topical agents with antifungal properties might be used in conjunction with systemic treatment in order to reduce the transmission of spores [1, 6].
In inflammatory cases, oral and/or topical corticosteroids may be considered in order to speed reduction of the inflammatory process. Their use is controversial, since some studies have shown that they do not reduce clearance time [1, 6]. Keratolytic emollients may be useful to remove crusts [1].
Follow-Up
Suitable Strategies
Eliminate viable spores in combs and brushes with an aqueous solution of 2% sodium hypochlorite, or hot water (>100 °C).
The index cases caused by T. tonsurans are highly infectious, so all close contacts should be examined.
Children can resume their school activity when systemic and topical treatment is initiated [1, 6].
Alopecia Areata
Alopecia areata (AA) is an autoimmune disorder. Up to 60% of the patients present their first episode before 20 years of age [1, 13].
Poor prognostic factors in patients with alopecia areata
Onset before puberty |
Positive family history |
Long-standing disease |
Nail involvement |
History of atopic dermatitis |
Association with Down syndrome |
Concomitant autoimmune disease |
Extensive hair loss (AA totalis/universalis) Ophiasis pattern |
AA may be associated with other autoimmune diseases in about 16% of the cases. Common associations are thyroid disease and vitiligo [1, 13].
Diagnosis
Clinical features: nonscarring alopecia – the most frequent pattern is patchy alopecia. Approximately 5% of the patients with this pattern will progress to alopecia totalis or universalis [1, 12].
Trichoscopy: black dots, exclamation mark hairs, broken and dystrophic hairs are markers of disease activity. Yellow dots are seen in chronic cases [14].
Histology: Avoid biopsies in children; trichoscopy allows diagnosis.
Management
Main topical and intralesional treatment options for alopecia areata
Agents | Indication | Side effects | |
|---|---|---|---|
Superpotent steroid | Clobetasol propionate 0.05% Start 3×/week and increase to 5×/week if no local side effects. | First line in children <10 years AA <50% scalp involvement Active/stable disease | Folliculitis, telangiectasia, and skin atrophy Avoid occlusion in children as it can cause adrenal suppression |
Irritants | Anthralin 0.5–1% cream Initiate: 20–30 min/day 5- to 10-min increments weekly, up to 1 hour (or until mild irritant reaction) Up to 1 year of treatment might be necessary to achieve response | Irritation, stinging, and brown staining of the scalp and clothing | |
Immunotherapy (contact sensitizers) | Diphenylcyclopropenone or squaric acid dibutylester solution | Long-standing or stable disease | Vesicular, bullous, or urticarial reactions, dyschromia, regional lymphadenopathy |
Intralesional corticosteroids | Triamcinolone acetonide 2.5–5.0 mg/ml | Age >10 years <50% scalp involvement | Pain Telangiectasia, depigmentation, and skin atrophy |
Other topical agent | Topical minoxidil 2–5% 1–2×/day | Adjuvant therapy | Contact dermatitis (minoxidil solution: propylene glycol) and hypertrichosis |

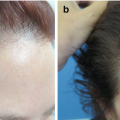
Young girl presenting diffuse hypertrichosis over the back after the use of topical minoxidil applied to the scalp. Parents referred applying minoxidil above the prescribed amount
Other topical treatments with varying results have been described in anecdotal reports including retinoids such as bexarotene 1% [27] and prostaglandin analogs [28, 29]. Calcineurin inhibitors are not effective. Topical Janus Kinase (JAK) inhibitors represent a promising therapeutic option, particularly for pediatric patients with AA refractory to other treatments. A small series of cases in this age group has recently been reported (2% tofacitinib and 0.6%, 1%, 2% ruxolitinib cream) with favorable results [24, 25].
Intralesional steroids can be used, although painful for patients over 10 years old, with patchy AA involving less than 50% of the scalp [16, 18, 23]. Triamcinolone acetonide is the most commonly used drug at 6-week intervals. Chu et al. observed that the concentration of 2.5 mg/ml confers the same benefit as 5 or 10 mg/ml with decreased incidence of local side effects [30]. For detailed information regarding therapy with intralesional steroids, refer to Chap. 2.
Systemic Treatment
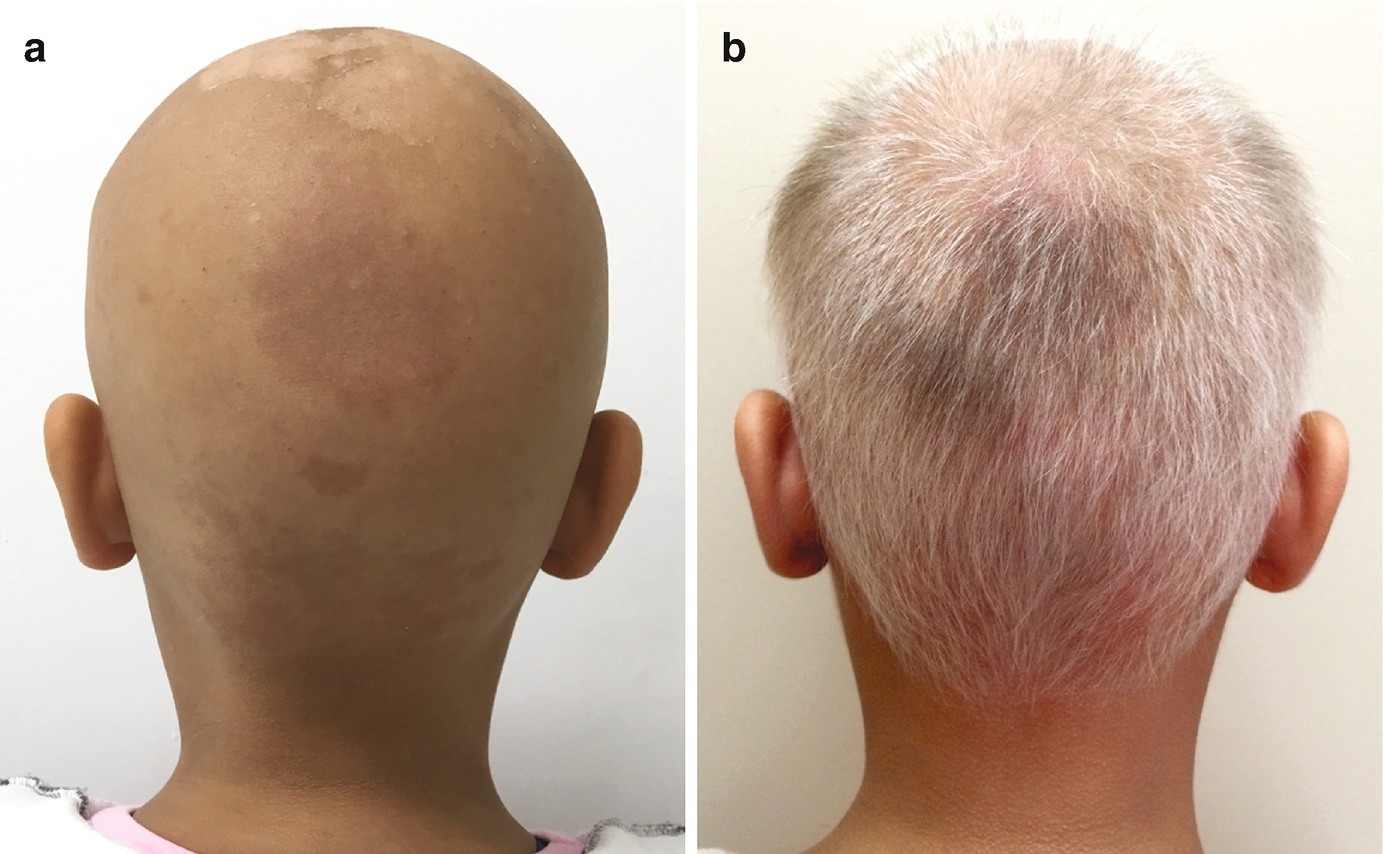
Seven-year-old girl with alopecia areata universalis (a) before and (b) under treatment with pulse corticosteroid therapy. Skin peeling in the first picture is secondary to sunburn and not related to the condition. Note that regrowing hairs in (b) are mostly white, a characteristic phenomenon in alopecia areata
Methotrexate represents a therapeutic alternative, but its efficacy in children is variable. A retrospective study evaluated 14 children with severe AA, who received doses of 15–25 mg once a week. A successful response (regrowth >50%) was seen in five patients and started at about 3–6 months [35].
Oral JAK inhibitors interfere with the JAK pathways, reducing the production of several inflammatory cytokines [16]. They have been shown to be effective in recent case series of AA in children. The main concerns are in regard of potential side effects, and additional evidence is still needed [12, 16, 23].
Phototherapy
Excimer laser (308 nm) may be helpful in limited patchy AA [18].
Psychiatric evaluation should be considered, owing to the higher prevalence of depression and anxiety in pediatric patients with AA [12].
Trichotillomania
Trichotillomania (TTM) consists of pulling out one’s hair. It is classified as an obsessive-compulsive disorder (OCD) in the fifth edition of Diagnostic and Statistical Manual of Mental Disorders. The scalp is the most frequently affected place; however, the eyebrows, eyelashes, and pubic hair may also be involved. TTM is seven times more common in children, with two peaks of initiation: 0–5 years (when it is a habit disorder, carried out unconsciously/automatically) and between 10 and 13 years. In this latter group, patients commonly report feelings of anxiety and distress that are only relieved by the act of pulling the hair [1, 16, 36].
Diagnosis
Clinical features: irregular patchy alopecia, hairs of different lengths, and excoriations. Hair pull test is negative. When localized to eyelashes, it only involves upper eyelashes [16, 37].
Trichoscopy: irregularly broken hairs, V-sign, flame hairs, coiled hairs, tulip hairs, and hair powder [38]
Histology: Performed only in doubtful cases. It is characterized by alternating damaged and intact hair follicles and absence of peribulbar inflammation. Signs of damage include trichomalacia, peri- and intrafollicular bleeding, and pigment casts.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


