div class=”ChapterContextInformation”>
8. Adherence in Atopic Dermatitis
Keywords
AdherenceAtopic dermatitisTopical corticosteroidsTopical calcineurin inhibitorsMoisturizersWet-wrapsCrisaboroleEducational workshopsWritten action plansRemindersAccountabilityIntroduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease that begins early in childhood and persists until adulthood. AD affects up to 11% of children in the United States and 20% worldwide [1, 2]. With impacts on sleep and social and intellectual development, AD can cause children and families to have a diminished quality of life. AD is a multibillion dollar problem to society, with an estimated direct cost of $900 million per year in the United States [3].
Management involves a variety of topical therapies including topical corticosteroids (TCS), topical calcineurin inhibitors (TCI), and emollients. When topical therapies fail, phototherapy and systemic treatments are initiated. Phototherapy can be an inconvenient option, whereas systemic treatment with prednisone, methotrexate, or cyclosporine can have long-term toxicity. Combating the burden of this disease requires a sophisticated approach, but treatment plans often compromise adherence to treatment. About 30% of AD patients do not take their medications as prescribed [4]. Research on the factors that affect patients’ adherence to treatment also has the potential to vastly improve patients’ outcomes and to do so quickly and at low cost. Nonadherence can be due to primary nonadherence, where patients fail to redeem their prescriptions, or secondary nonadherence, where patients do not take their medication as directed. This chapter will look at the prevalence of nonadherence in AD patients, barriers to adherence, and potential interventions for this subset of patients.
Prevalence of Nonadherence in Atopic Dermatitis
Numerous studies have assessed adherence rates in AD. A study assessed primary nonadherence in 322 subjects at an outpatient dermatology clinic. They analyzed the frequency of prescriptions filled within 4 weeks of their appointment. Of 137 AD subjects given a new prescription, 31.4% did not redeem their prescriptions [5].
Once patients fill their prescriptions, many patients still do not take their medication as directed. In one study, only 50% of patients initiated treatment during an acute AD flare with an average treatment delay of 7 days [6]. For long-term management of AD, many patients fail to use the proper amount of medication. Patients may underuse or overuse medications leading to insufficient treatment response. In a study evaluating the efficacy of a topical tacrolimus in adult AD subjects, 66.7% underused the prescribed medication, 12.4% overused, and 20.9% used the proper amount [7]. Those who underused the recommended treatment reported poorer improvement in Eczema Area and Severity Index (EASI) score than those who used the proper amount of medication (1.64 vs 4.65) [7].
Despite high self-reports of adherence by patients, the adherence rate as measured by electronic monitoring is far from perfect. Of 25 AD patients using twice daily hydrocortisone 17-butyrate 0.1% in one of three vehicles, 70% adhered to the medication despite nearly all patients self-reporting perfect usage of the medication [8]. Another study involved 41 subjects with mild-to-moderate AD who were instructed to use desonide hydrogel 0.05% twice daily. Mean adherence declined over time from 81% on day 1 to 50% by Day 27 [9]. Although self-reported adherence rate was 87% among AD subjects using clocortolone pivalate cream 0.1% at Week 4, the average adherence rate determined by electronic monitoring was 70% [10].
Even short-term treatment results in poor adherence. When 10 subjects with mild-to-moderate AD were instructed to apply fluocinonide cream 0.1% twice daily for 5 days, the mean adherence rate measured by electronic monitoring was 40% [11].
There is a high prevalence of nonadherence in AD as assessed by clinical trials evidence. Furthermore, adherence rates are often overestimated in clinical trials so there is concern that adherence is much poorer in clinical practice. Poor adherence may explain suboptimal treatment response and therefore should recognized and addressed before switching to a more harmful medication.
Nonadherence Goes Beyond Topical Corticosteroids
Topical corticosteroids are first-line treatments for AD. Much of the data on adherence comes from the use of these topical agents; however, there are a variety of other topical therapies that are used in AD that may also present challenges to adherence. These include moisturizers, wet-wrap therapy, topical calcineurin inhibitors, and topical phosphodiesterase 4 inhibitors.
Moisturizers
Daily moisturizer use is standard of care treatment for AD prevention and maintenance therapy [12]. Moisturizers include emollients, humectants, and occlusive agents. Nonadherence may be an issue if these agents misalign with patient preference and cause inconvenience. The most commonly cited reasons for nonadherence to moisturizers are skin discomfort (27%), time-consuming application (22%), and cost (23%) [13]. Although providers prefer creams and ointment moisturizer vehicles due to their effectiveness, their thicker consistency, in contrast to lotions, may impede adherence. Occlusive agents are very greasy, have a strong odor, contain potential allergens, and cause folliculitis when inappropriately used [14]. AD patients prefer a moisturizer based on “consistency,” whether it “absorbs fast,” and is “nice to wear.” [15].
In addition to inconvenient moisturizer application, 23% of AD patients believe that moisturizers play a minimal role in managing eczema [13]. About 75% of AD caregivers believe emollients provide short-term relief but there are barriers for long-term use [16]. Some caregivers believe emollients are “unnatural,” contain “chemicals,” and the skin gets “used to emollients” thus losing effectiveness with regular use [16]. Patient belief is a large barrier to nonadherence. Although most caregivers agree emollients help with active disease, some reported mixed feelings when using emollients during disease remission [16].
Wet-Wrap Therapy
Wet-wrap therapy is indicated for severe or refractory AD [12]. Wet-wrap therapy consists of a wet layer of occlusive bandages followed by dryer outer layer. Wet-wrap therapy increases contact time with topical therapies resulting in increased absorption. Due to its messiness, inconvenience, feasibility, and time-consuming application, it may be a less attractive option for children and caregivers. Other common adherence barriers to wet-wrap therapy include high cost, special training in usage, unpleasant sensation of cold damp wraps, increased risk of cutaneous infection , and poor tolerability [17].
Topical Calcineurin Inhibitors
Topical calcineurin inhibitors (TCIs) are second-line therapies, appropriate for thin and sensitive skin that may not tolerate TCS. TCIs include tacrolimus ointment (0.03% for patients over 2 years and 0.1% for patients >15 years) and pimecrolimus cream (1% for patients >2 years) [12]. Tacrolimus is Food and Drug Administration (FDA)-approved for moderate-to-severe AD whereas pimecrolimus is approved for mild-to-moderate AD. Common side effects of TCIs include burning and stinging; the label contains a black box warning for potential malignancy. The black box warning may raise concerns that impede patient adherence, even though there is considerable evidence that topical calcineurin inhibitors do not cause an increased risk of cancer. A study assessed adherence in 200 AD patients who were instructed to apply topical tacrolimus twice daily; the average number of applications per day was 1.75 ± 0.53 and there was a steep decline in adherence from the first to second week (73.5% vs 61%) [18].
Topical Phosphodiesterase 4 Inhibitors
Crisaborole has been recently FDA-approved for mild-to-moderate AD in patients 2 years and older. Although crisaborole does not have the adverse effect profile of topical corticosteroids, application site pain is a common finding that may impede adherence [19]. Other reasons for nonadherence include high cost and slow onset of action.
Barriers to Adherence
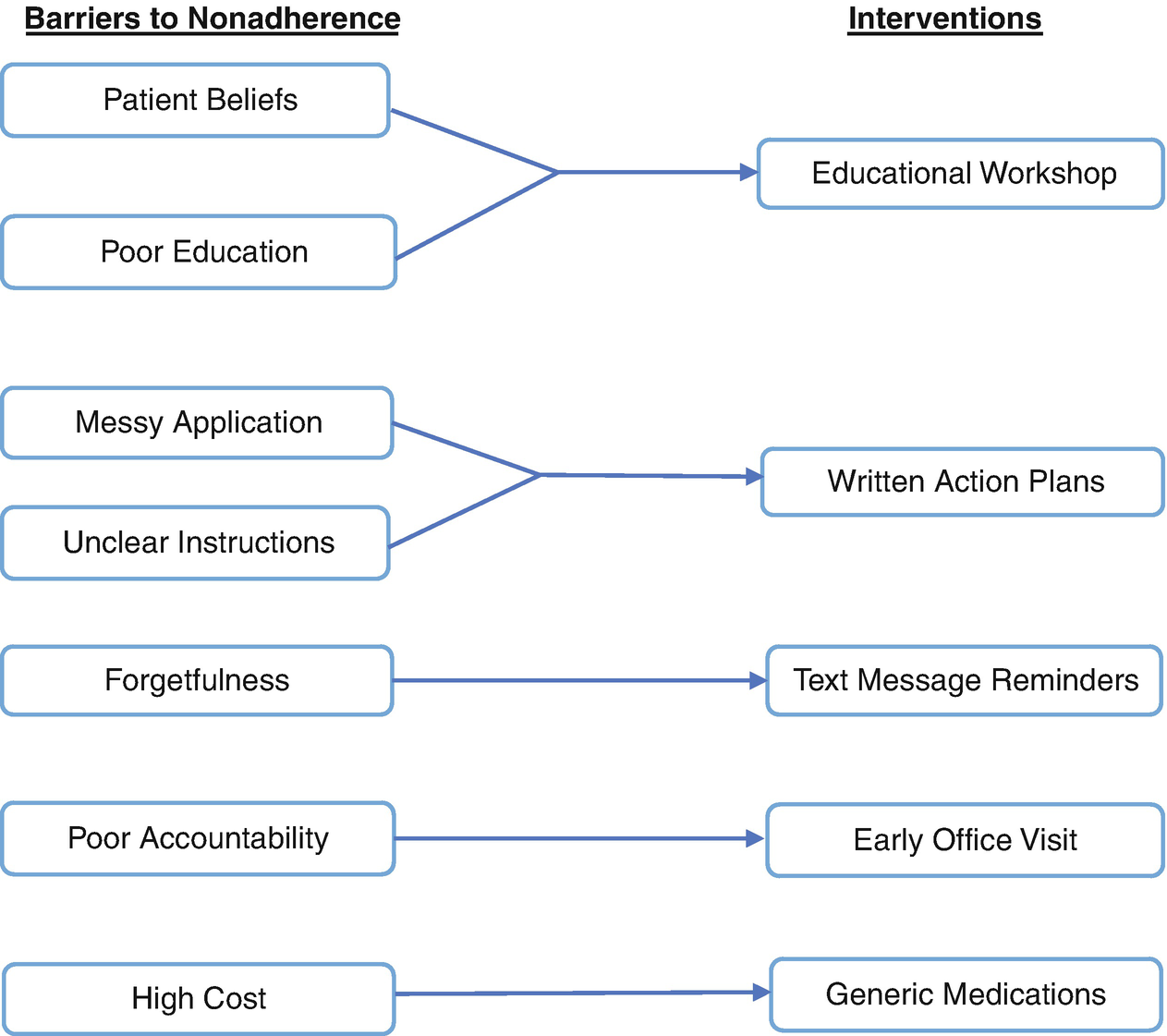
Knowledge Gaps and Fears of Adverse Effects
Often, patients may not be fully aware of the benefits of moisturizers and adjunctive therapies such as TCI in managing AD and fear the risks of TCS [22]. In a survey of caregivers with children suffering from dermatological conditions, the most commonly cited concern about medication use was a fear of side effects [23]. Of 208 AD patients, 80.7% reported fear of TCS. There was a positive correlation between the fear of TCS and the belief that topical corticosteroids pass through the skin into the bloodstream (B-coefficient = 0.63, P < 0.001), inconsistent information about the quantity of cream to apply (B-coefficient = 0.34, P < 0.05), and poor treatment adherence (B-coefficient = 0.53, P < 0.05) [24]. Of 77 caregivers, 64% reported that they worry a lot about using topical corticosteroids on their child. Caregivers most frequently worry over skin atrophy [25].
Poor Communication
Poor communication and misalignment with patients’ preferences are common impediments to adherence. Patients may be confused about the different potencies of TCS and how to appropriately apply the medication [26]. In a survey identifying reasons for nonadherence to topical therapies, 18.2% reported unclear instructions as a common barrier to optimal management [27]. With complex treatment regimens, only 24% of AD caregivers feel confident they can manage AD flares and 75% felt that the most important determinant in their child’s quality of life was effectively controlling their AD [6].
Patients may prefer some types of treatments over others in order to minimize inconvenience arising from messy application, strong odor, and time-consuming regimens [22]. Patients may also prefer a particular type of vehicle in regards to topical corticosteroids and moisturizers [9, 28].
Forgetfulness
Forgetfulness is a common cause of unintentional nonadherence, especially in chronic diseases like AD. About 80% of nonadherent subjects attribute poor adherence to forgetfulness [27]. To address forgetfulness, incorporating required medications into an existing daily routine may help. One approach might be to apply the medication every morning after breakfast [29]. Pediatric AD patients may benefit from sticker calendar charts. A sticker is placed on each day of the calendar following appropriate use of the medication providing positive reinforcement and a reminder for the next dose [30].
Adherence Interventions for Atopic Dermatitis
Interventions for improving adherence in atopic dermatitis patients
Author | Study design | Intervention | Number of subjects | Primary outcome | Result |
|---|---|---|---|---|---|
Educational workshops | |||||
Grillo et al. [31] | RCT | 2-hour educational workshop | 61 | SCORAD | Intervention:53.9% vs control: 15.8%; P < 0.05 |
IDQLI, CDLQI, DFI | No difference between groups | ||||
Moore et al. [32] | RCT | Nurse-led educational workshop | 99 | SCORAD | Intervention: 73% vs control: 40%; P < 0.001 |
Staab et al. [33] | RCT | 6 sessions of 2-hr educational workshops | 204 | SCORAD | No significant difference between groups; P = 0.43 |
Treatment habits-use of TCS | Intervention: 65% vs control: 38%; P = 0.041 | ||||
Shaw et al. [34] | RCT | 15-minute educational workshop | 106 | SCORAD | No significant difference between groups |
IDQLI | No significant difference between groups | ||||
Chinn et al. [35] | RCT | 30-minute educational workshop | 235 | IDQLI | No significant difference between groups |
Written action plan | |||||
Rork et al. [37] | Non-RCT | EAP | 35 | Telephone survey 3–12 months later assessing disease severity and helpfulness of EAP | 68% of children improved from baseline and 86% found EAP helpful |
Gilliam et al. [38] | RCT | EAP | 88 | Childhood AD impact score-quality of life | No significant difference between groups |
Text messaging | |||||
Pena-Robichaux et al. [40] | Non-RCT | Daily text message reminders | 25 | Self-reported medication diary and self-reported forgetfulness in taking medication | 72% improvement in adherence compared to baseline; P < 0.001 |
Singer et al. [41] | RCT | Daily text message reminder | 30 | EASI | Intervention: 58% vs control:53%; P > 0.05 |
AD knowledge quiz | Intervention:84.6% vs control: 74.8%; P = 0.04 | ||||
Early follow-up | |||||
Sagransky et al. [43] | RCT | Early 1-week follow-up | 20 | Medication event monitoring system-adherence | Intervention:69% vs control: 54%; P > 0.05 |
EASI | Intervention: 76% vs control: 45%; P > 0.05 | ||||
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


