46
Ichthyoses and Erythrokeratodermas
• Clinical features that are useful in determining the type of ichthyosis include the time of presentation (e.g. at birth, ± a collodion membrane, vs. later in life), the quality and distribution of the scaling, other cutaneous manifestations (e.g. erythroderma, blistering, abnormal hair), and extracutaneous or laboratory findings (Table 46.1).
Table 46.1
Clues to the diagnosis of ichthyoses and erythrokeratodermas.
The disorders in this table are discussed in greater detail in the text or Table 46.2. Other rare ichthyoses and related disorders can also present with these findings.
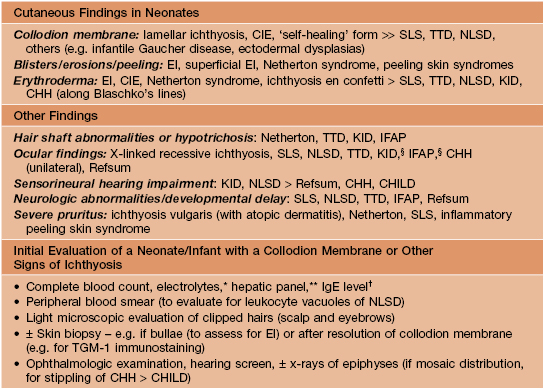
§ Keratitis has variable onset.
* Hypernatremic dehydration occurs primarily in collodion babies and neonates with Netherton syndrome, EI, or Harlequin ichthyosis.
** Elevated transaminases are common in NLSD.
† Increased in Netherton and inflammatory peeling skin syndromes.
CIE, congenital ichthyosiform erythroderma; CHH, Conradi–Hünermann–Happle syndrome; EI, epidermolytic ichthyosis; CHILD, congenital hemidysplasia with ichthyosiform nevus and limb defects; IFAP, ichthyosis follicularis with atrichia and photophobia; KID, keratitis–ichthyosis–deafness syndrome; NLSD, neutral lipid storage disease; SLS, Sjögren–Larsson syndrome; TGM-1, transglutaminase-1; TTD, trichothiodystrophy.
• A few ichthyoses have characteristic histologic features (e.g. epidermolytic ichthyosis; see below).
Ichthyosis Vulgaris (IV)
• The most common disorder of cornification, with a prevalence of at least 1 in 200.
• Mild to moderate scaling favors the extensor extremities (Fig. 46.1), ranging from fine white scales to larger adherent scales (especially on the lower legs); the trunk, scalp, and forehead are occasionally affected, and flexural sites are characteristically spared.

Fig. 46.1 Ichthyosis vulgaris. Fine white scales on the lower extremities. Courtesy, Julie V. Schaffer, MD.
• Associated findings include hyperlinear palms (Fig. 46.2), keratosis pilaris, and atopic dermatitis (25–50% of patients, ± other atopic disorders such as asthma and allergic rhinitis).

• DDx: xerosis, acquired ichthyosis, X-linked ichthyosis.
X-Linked Recessive Ichthyosis (XLRI; Steroid Sulfatase Deficiency)
• The underlying steroid sulfatase deficiency is caused by deletion of the entire STS gene on chromosome Xp22 in ~90% of patients; XLRI is occasionally part of a contiguous Xp microdeletion syndrome that also includes Kallman syndrome (hypogonadotropic hypogonadism with anosmia) and X-linked recessive chondrodysplasia punctata.
• Affected neonates may have generalized exfoliation of translucent scales, followed during infancy by the development of characteristic dark brown, polygonal, adherent scales favoring the neck, preauricular area, scalp (especially in young children), extremities, and trunk; the palms, soles, and flexural sites tend to be spared (Fig. 46.3).



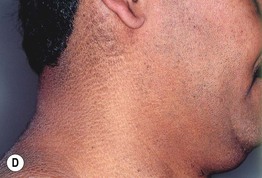
Fig. 46.3 X-linked recessive ichthyosis. Large light brown (A) and more prominent dark brown (B) scales on the lower leg. C Smaller dark brown scales on the trunk, with sparing of the skin folds. D Dark scales on the neck, sometimes referred to as a ‘dirty neck.’ A–C, Courtesy, Julie V. Schaffer, MD; D, Courtesy, Gabriele Richard, MD, and Franziska Ringpfeil, MD.
• Often improves substantially in the summer.
•






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


