The term “Hybrid” has recently come to designate an specific intermediate entity between Preservation and Structural techniques, with the tip being done structural and the dorsum by preservation. This limits the indications to patients who present aesthetically pleasant dorsums, which can thus be fully preserved. In my “modified dorsal split” approach, the dorsum is split anatomically and reshaped appropriately. I preserve the Dorsal Keystone Area while the middle vault is reshaped and adjusted, followed by a cartilaginous push down or a full symmetric or asymmetric let down. Thus, patient indications are significantly expanded.
Key points
- •
“Pure” pushdown/letdown dorsal preservation, which keeps the middle vault fully intact, is indicated only for those few patients who have aesthetic dorsal lines from the start.
- •
The middle vault must often be adjusted. Although surface modifications are sometimes enough, opening the middle vault is often beneficial.
- •
“Hybrid Dorsal Preservation” signifies for me opening the middle vault along the septal T and then using a cartilaginous pushdown or a full letdown procedure.
- •
The tip is then done structural with preservation/reconstruction of ligaments.
- •
The hybrid concept is further integrated by the specific use of Power and Piezo tools for separate, integrated indications.
Video content accompanies this article at http://www.facialplastic.theclinics.com .
Introduction and background
Since 2017 (my first case of cartilaginous pushdown), I progressively developed a strong interest in the mounting at first, and then overwhelming, tide of Preservation rhinoplasty. One could well state that preservation is now so widely accepted to be seen by many as the exclusive way to perform rhinoplasty today. The reason of my interest was the clarity of new anatomy concepts, the fascination with those attractive and logical principles of preserving specific structures without unnecessary destruction-reconstruction , and, not least, my direct friendship with eminent surgeons advocating preservation. At the same time, I was benchmarking with many years of structural practice with essentially good results. Thus, I was trying to honestly gauge whether embracing a new philosophy would be truly beneficial to my patients, apart from excessive and misleading marketing, while taking an acceptable toll from the related learning curve I had to go through. During this learning curve, aided by attending meetings, relating with colleagues, performing dissections, and developing a progressive experience, I progressively matured the conviction that the “virtue indeed lies in the middle”. Thus, I started using the term “hybrid rhinoplasty” which, to my knowledge, we first popularized in the Bergamo Open Rhinoplasty Course in March 2022. This paper will summarize my current concepts in employing a hybrid dorsal preservation approach to primary rhinoplasty, which essentially combines different techniques and different tools. Essentially, I believe that the time and the effort related to the learning curve are worth the trouble since the results are better. However, the subject is vast and at times not easy.
The key concept
The Merriam-Webster dictionary defines “hybrid” as “… produced by a combination of two or more distinct elements: marked by heterogeneity in origin, composition, or appearance ”.
Since the term is becoming popular in rhinoplasty and its significance varies from surgeon to surgeon, this is what I currently mean by “hybrid” rhinoplasty:
- 1.
The tip is done structurally open with recognition (preservation or reconstruction) of ligaments. This will be outside the scope of this paper. The dorsum is, however, not purely preserved as is, but is “hybridized”. The DKA is preserved, while the middle vault is split anatomically and adjusted as in component separation. A cartilaginous pushdown (“surface” technique) or a full letdown (“foundation” technique) will then follow, depending on the shape and height of the bony cap.
- 2.
Power and Piezo tools are used both for specific and integrated indications. Again, this is a hybrid mixture of different tools, which can work perfectly well together, each being used for a preferred purpose.
The premise behind this thinking is that only few dorsums can be managed by a pure preservation approach. In my practice, only 15%–20% of primary patients have ideal dorsal lines, and thus a dorsum that is so aestheticallypleasing to be left as is. Interestingly, several colleagues are now employing hybrid variations with surface modifications added to the dorsum. This usually requires some reshaping of bone and cartilage, thus some surface modifications, but still keeping the middle vault intact, and consequently necessitating release of the lateral keystone area (LKA) for efficiently lowering the hump.
In 2017, we highlighted the distinct anatomy of the septal T , which can be also designated as “T-bar”, and its use as an anatomic graft to the tip in structural rhinoplasty, following component separation and incremental reduction. The term “Septal T” indicates the T-shaped dorsal portion of the septum which includes, as a single unit, both a vertical portion of septum as well as its two transverse limbs on either side. These transverse limbs serve a relevant purpose to the inner nasal valve, are pertinent to the septum, and continue by flowing laterally into each upper lateral cartilage. The limbs of the Septal T represent the flared dorsal border of the quadrangular cartilage, which become visible after they are detached from the upper lateral cartilages along a plane that is anatomically distinct and easily viewable in most cases. The shape of the septal T dictates the shape of the nasal dorsum, starting at the end of the bony cap together with its frequent asymmetries, and contributes to its width. Opening the middle third of the nose along the edges of the septal T is thus different from splitting the middle vault with a vertical cut flush to the septum.
The next step became, logically, to split the middle vault identically while preserving the dorsal Keystone area, strategic and difficult to reconstruct in a structural approach.
We initially applied this concept as a cartilaginous pushdown approach, a surface technique not dissimilar from what described by Ishida and Ferreira, but with the fundamental difference of using an open approach and splitting the middle vault, The next step, in the presence of bony caps of greater significance, then became that of performing a full letdown, either symmetric or asymmetric, still by opening the middle vault, preserving the DKA, trimming the excess of the upper laterals, and reshaping middle vault asymmetries. In both cartilaginous-pushdown and full-letdown procedures, the middle vault would then be closed anatomically along the septal T.
We currently apply modified dorsal split hybrid preservation techniques in about 80% of our primary cases. In the rest, the dorsum is managed by a structural approach. Notably, our primary patient population is highly varied in morphology and age and currently comprises about 30% – 35% male patients.
The rationale
The following points are my key principles in the two main varieties of cartilaginous pushdown and full letdown modified dorsal split hybrid preservation techniques.
- 1.
Preserving the most delicate structure which is indeed the most difficult to reconstruct, that is, the DKA.
- 2.
Maintaining an option B (safety net): converting to a structural incremental reduction is still possible after a component separation with a middle vault split along the septal T.
- 3.
Understanding that in many cases the bony hump is minor and the cartilaginous hump major. Surface techniques will work well here.
- 4.
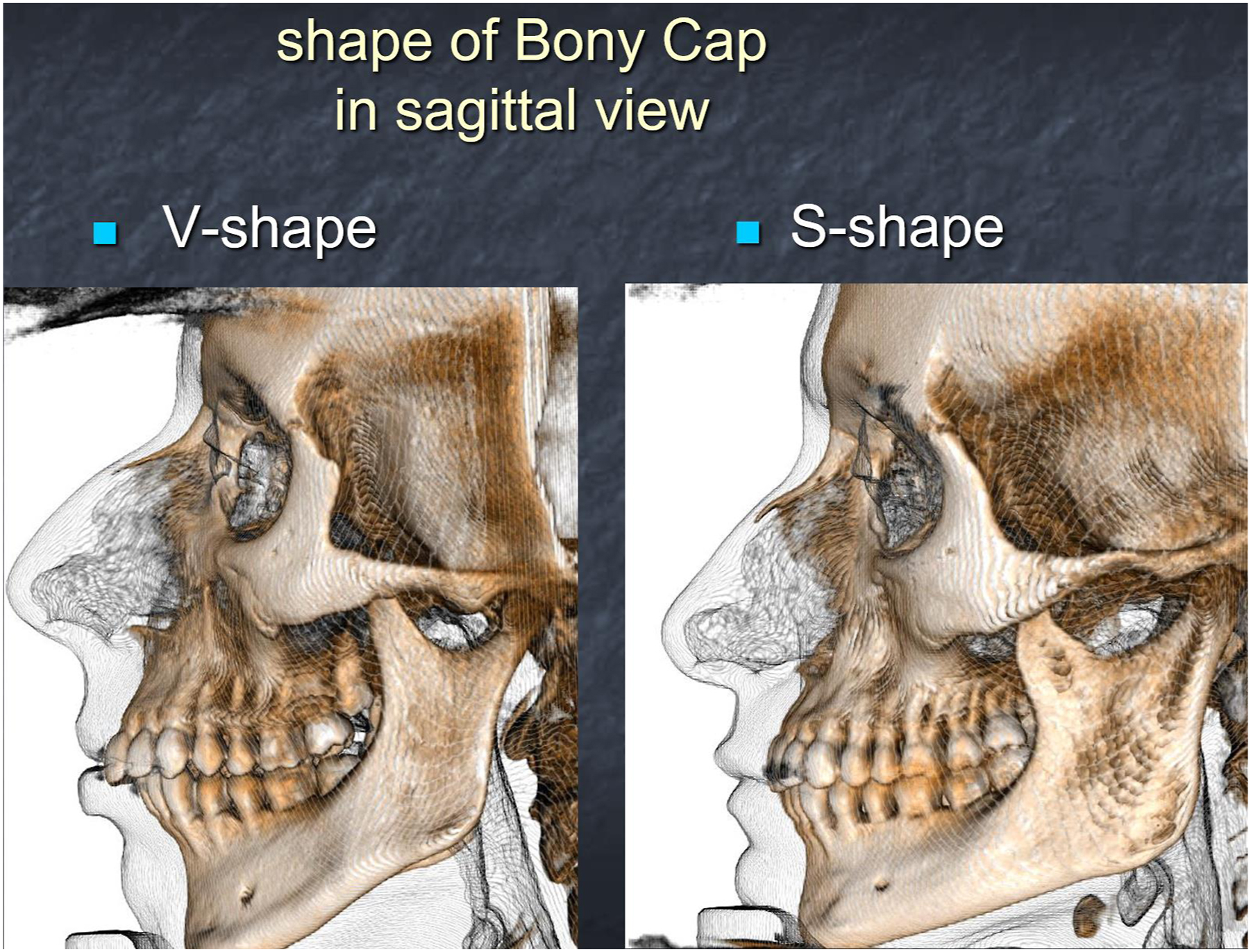
Converting some more relevant bony humps to lesser bony humps, by reducing their height, as well as by defining their shape from S-shaped to V-shaped, through the use of Power tools and Piezo. Then, surface techniques will still be employed, possibly including a portion of the bony hump in the pushed-down DKA (Furtado-Khazaal modification).
- 5.
Using full letdown, symmetric or asymmetric, technique for significant bony humps. Foundation techniques will be necessary here.
- 6.
Preferring the superior-middle strip approach (Most-Patel) due to the familiarity of the L-strut concept and the greater availability of grafting material in most (not all) cases.
In addition to what is stated above, there are some further common ingredients which matter:
- a.
Using an open approach. I invariably use an open approach since I want to see those areas where work is done
- b.
Fully exposing my dorsum. This is because in almost every case I have to reshape my dorsum to some degree to improve the dorsal aesthetic lines. Leaving the dorsum undissected is an attractive idea that could be indicated in a small minority of my varied patient population. Also, I often have to redrape the skin envelope when the skin is redundant, and thus, a full degloving works best in my hands.
- c.
Using Piezo as an instrument to cut the bone
- d.
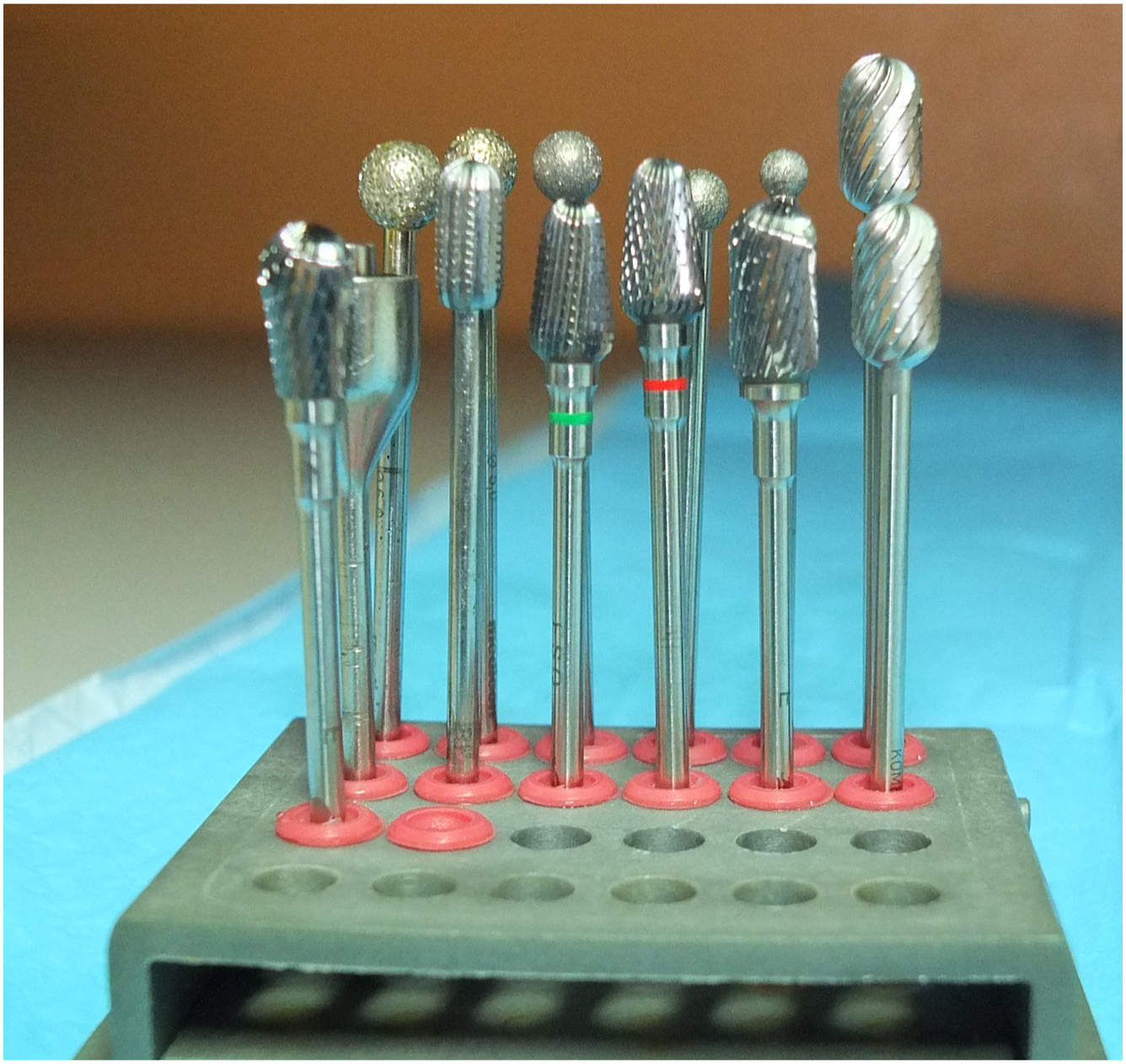
Using Power as an instrument to reshape bone: I use either flat (conical, reverse conical or cylindrical) burrs, round burrs, or disc-shaped burrs for different indications.
- e.
Using a cone beam computerized tomography (CT) scan (CBCT) for diagnosing the type of hump and the shape-inclination-thickness of the nasal bones.
- f.
Adding some elements, which are the same that I currently employ even in the structural approach: supraperichondrial dissection on the lower lateral cartilages, progressing subperichondrially at the vertical scroll, 3-points compartmentalization, drains, sidewall laminas
The Cartilaginous Pushdown Modified Dorsal Split Option
The bony cap is lowered by osteoplasty only, by Piezo or Burr, together with conventional osteotomies in wide nasal bones. The upper lateral cartilages are separated anatomically from the edges of the septal T, and the width and symmetry of the middle vault are adjusted. “Pedestal” spreader grafts can be added as needed, differentially shaped or unilateral if necessary. Resection of a high-middle septal strip allows pushdown of the DKA at the keystone junction. Septal deviations can be corrected according to the L-strut principle, with care in leaving a solid septal L strut which thus represents a comfortable safe zone when one is accustomed to structural concepts. Frequently, a vertical split Vitruvian man maneuver is employed for flexing the chondro-osseous junction at the DKA area The cartilaginous dorsum is then sutured into position under direct vision, in an end-to-end or end-to-side fashion (to compensate minor residual deviation as well as improve stability) and the middle vault is reconstituted by resuturing the septal T to the upper lateral cartilages after appropriate trimming of the edges of the upper lateral cartilages or/and of the Septal T itself.
This technique essentially combines the popular component-separation principle with the preservation of the delicate anatomy of the dorsal keystone area, while allowing modifications of the middle vault. Further details can be found in our publications The best indications for this technique are in patients with a bony hump measuring usually less than 3 mm. This is not uncommon, since prevalently cartilaginous humps are seen quite frequently. What we have added in recent years to this technique is a more liberal use of burrs. Flat-shaped burrs as well as conical and reverse-conical burrs, according to the need, are used at low revolutions per minute (below 10.000 rpm) and with ice-cold solution to shape bone efficiently and rapidly. The use of Piezo is mainly limited to the possible resection of an ethmoid component of the high-middle septal strip as well as to the possible, conventional, additional osteotomies. Those can be stabilized by transosseous sutures, as described by Gubisch and Haack, if it is felt that proper stabilization is helpful. As popularized by some South American surgeons, we have also found that the delicate use of pinpoint cautery can finely, directly reshape minor contour deformities of the cartilage.
An interesting modification of this technique, still based on a high or high-middle strip, has been described independently by Sergio Furtado and Ali Khazaal. It essentially expands the indications of the cartilaginous pushdown by including a portion of the bony cap, defined by precise, paramedian piezo cuts, and ostectomy of triangular bone wedges, together with the pushed-down DKA. The edge of the upper lateral cartilage can then be used as an autospreader flap. This has several points in common with Ferreira’s spare roof type B technique. Once again, however, it is done by an open approach and after splitting the middle vault.
A further modification of the same technique has been independently described by Sousa Vieira. A low strip is used here and the upper lateral cartilages are again used as autospreader flaps.
Interestingly, the same concept can be used endonasally, with a low strip approach, as described by Baris Cakir.
All the variations mentioned above essentially share the same principle of splitting the cartilaginous dorsum along the septal T, recreating new dorsal lines by surface modifications both by cartilage adjustments and by use of Piezo and Burrs, avoiding LKA release, and finally, resuturing the upper lateral cartilages to the septal T to rebuild the middle vault.
The Full Letdown Modified Dorsal Split Option
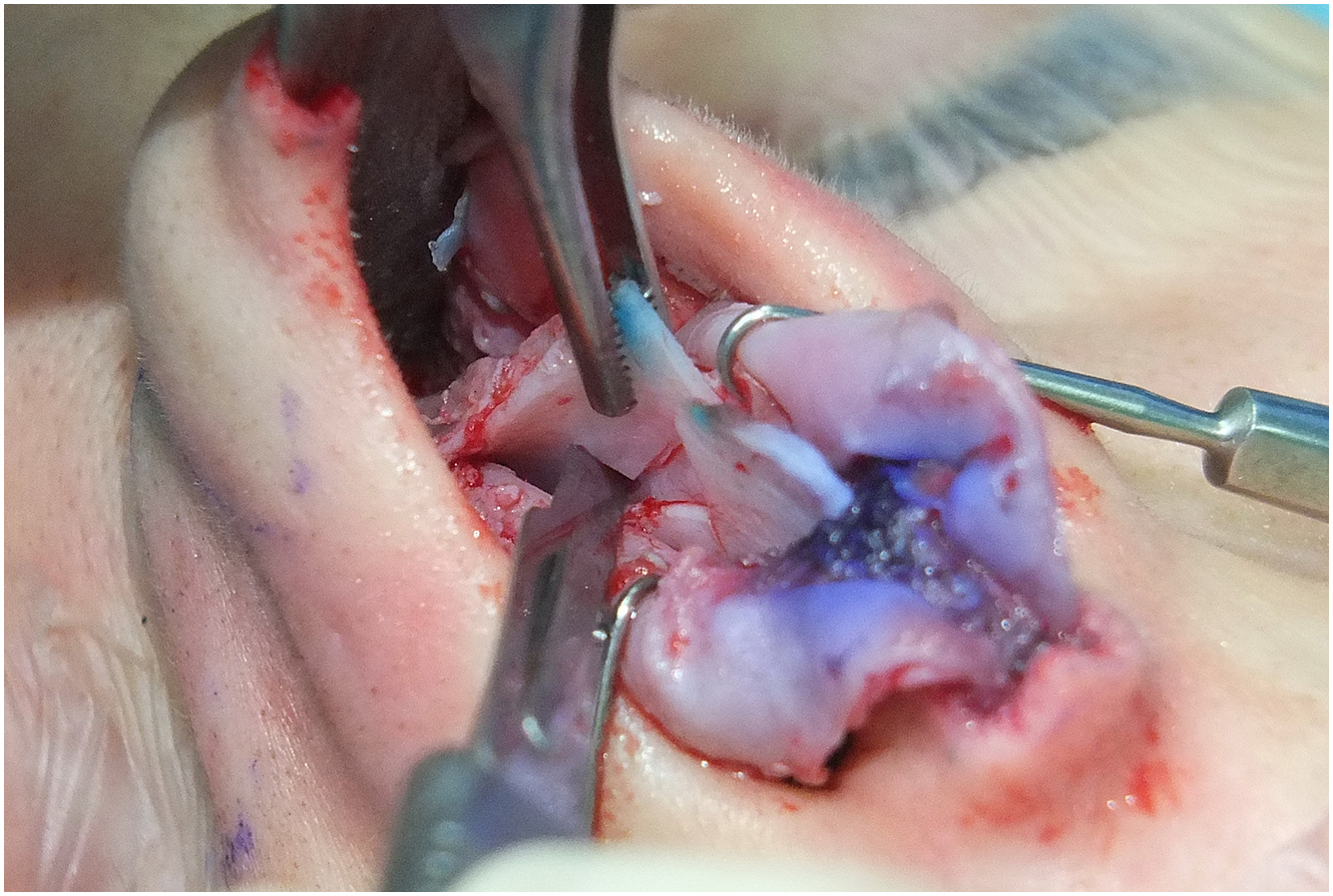
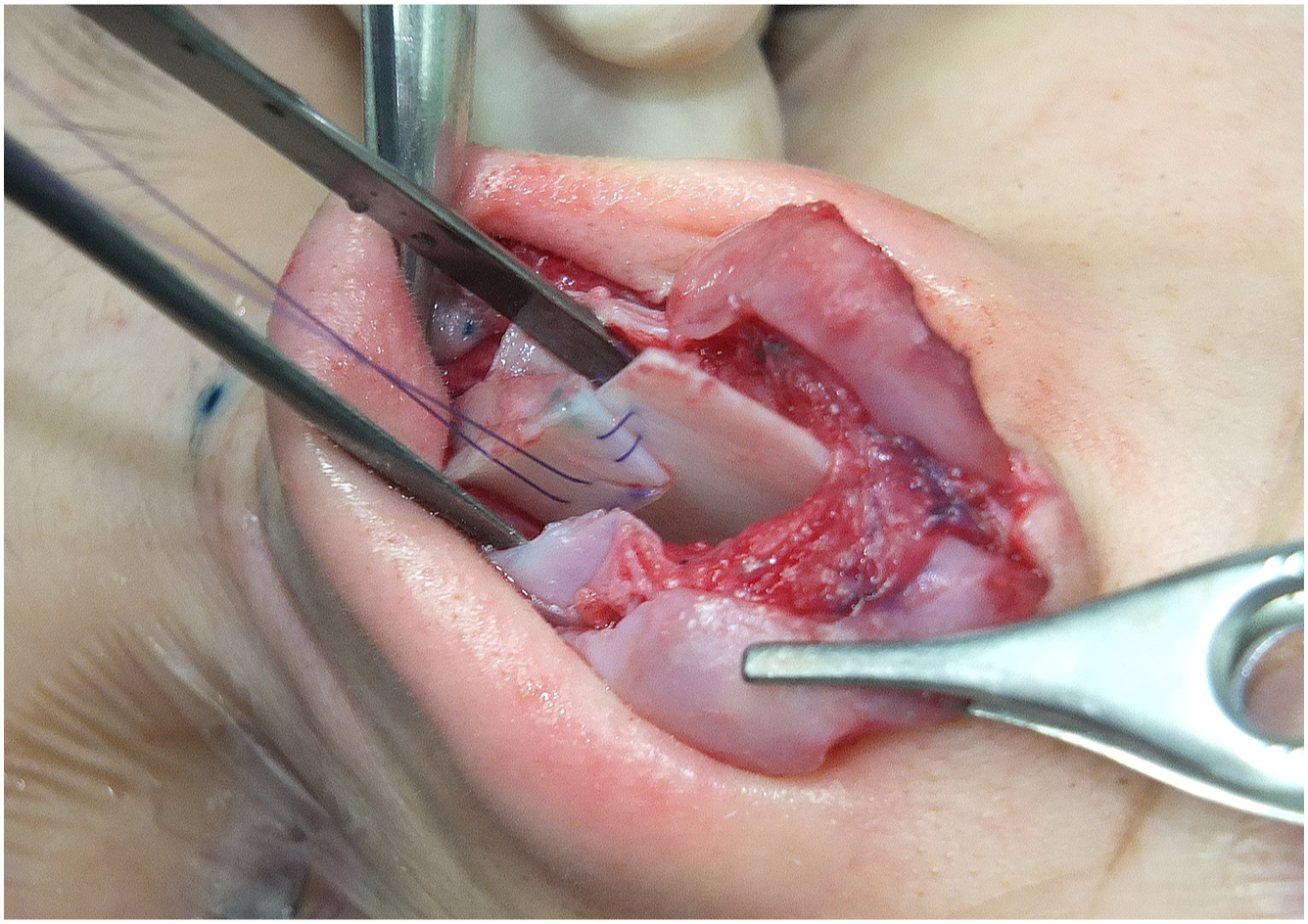
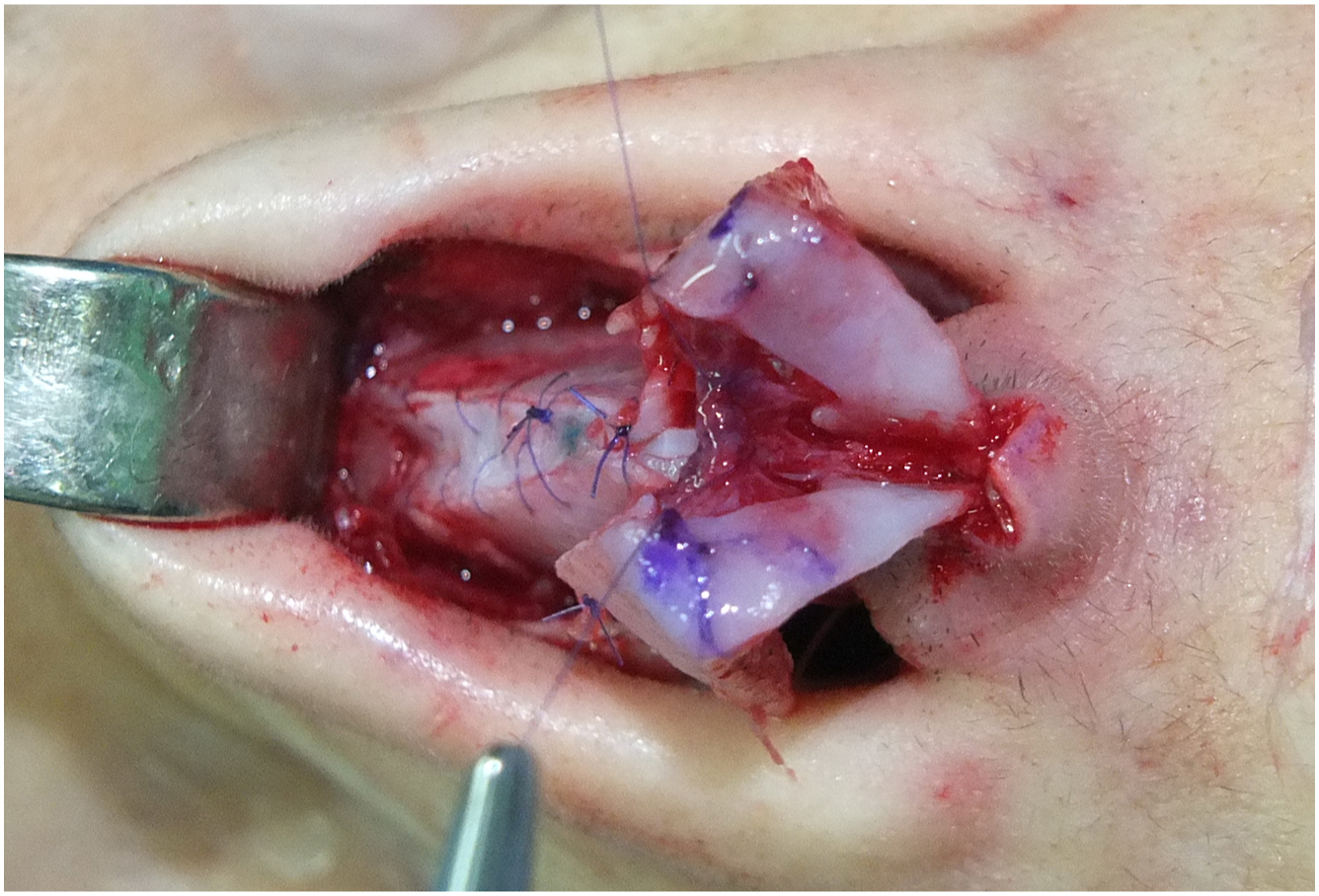
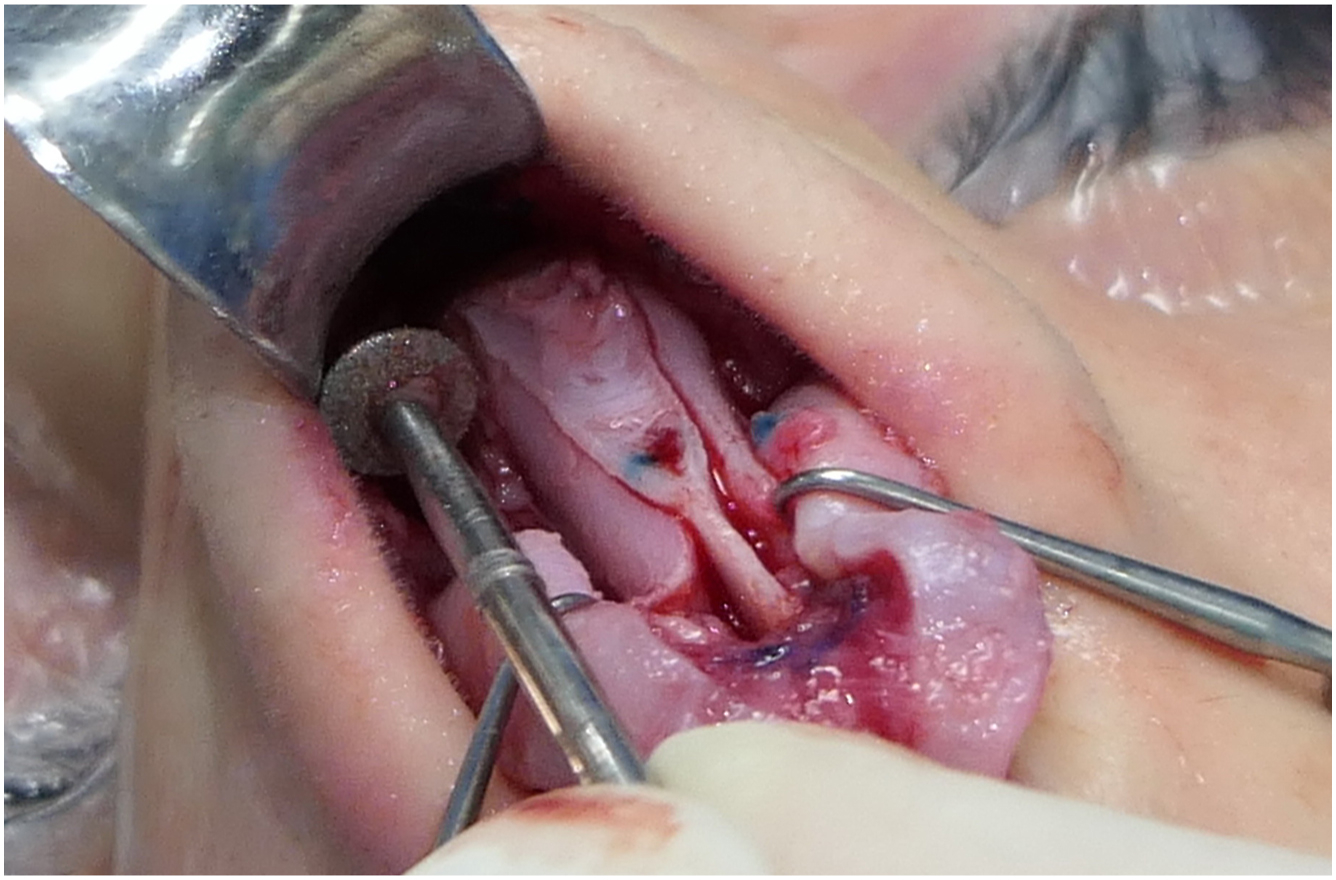
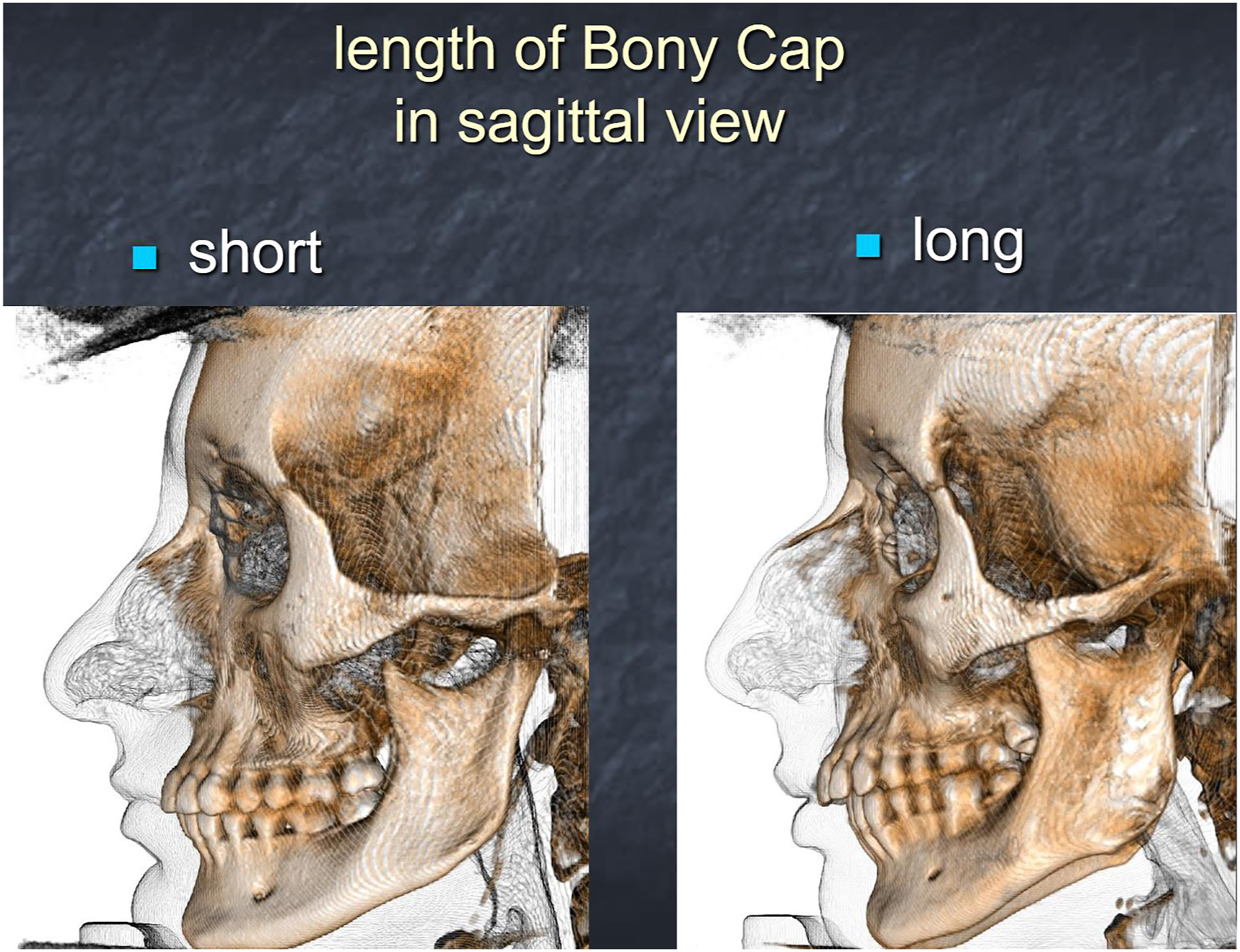
The dorsal split preservation concept of splitting the middle vault along the paraseptal cleft on the edge of the septal T and preserving the delicate DKA area while reshaping the middle vault can well be extended to full letdown techniques ( Figs. 1–3 ) (Please see [CR] ). This will broaden the indications to significant dorsal humps which cannot be managed by osteoplasty of the bony cap followed by a cartilaginous pushdown. Even S-shaped significant bony humps, which seem to negate the possibility of a letdown, can often be addressed by first converting the S-shape to a V-shape by osteoplasty and then proceeding to a full letdown. The middle vault is split on an anatomic plane along the septal T, the DKA is maintained, the middle vault is reshaped, similar to what was described in the cartilaginous pushdown, the septum is addressed by conventional L-strut septoplasty, a high-middle strip is used and precise direct suture fixation under vision easily accomplished. However, Piezo circumferential osteotomies will be necessary. Depending on the shape and inclination of the nasal bones, the letdown will be symmetric or asymmetric, with differential resection of wedges of bone. The use of Piezo will be instrumental here as a uniquely efficient bone-cutting tool. Regarding the transverse cut at the radix, my recent preference has been to employ a fine disc burr under direct vision, although this will mean fully exposing the radix ( Fig. 4 ). Performing this maneuver with care while combining with fine segmental progressive excision of ethmoid wedges below will avoid an excessive drop of the radix in most cases, although some osteoplasty at the step-off may be necessary. The alternative choices of a correctly-oriented oblique radix osteotomy from the outside with a 2 mm osteotome or of a Piezo-led osteotomy from the inside are interesting options. Another alternative can be the use of Piezo insert via a small external incision if proper care of the skin is taken. My feeling is that those options will be less precise, although they will allow the maintenance of some perichondrium at the radix attached to the skin, thus limiting the occurrence of an excessive drop.
Hybridizing further: combining Piezo and power tools: why and where
My current concept on hybrid management of the dorsum goes beyond the blend between structural and preservation techniques, since it also combines the use of both Piezo and power tools ( Fig. 5 ). Different surgeons have used either of those, highlighting their advantages, but in practical terms, selectively and mutually exclusively. Over the last few years, we have integrated efficiently the use of Piezo, which has gained great popularity over the last few years, after being pioneered by Olivier Gerbault, to the use of power tools, which had been introduced much earlier in rhinoplasty. Recently, several surgeons have convincingly demonstrated the use of diverse new burrs. By progressively selecting and adopting specific spherical, cylindrical, conical, and discoid tips, it became clear to me that such burrs can be used logically and effectively, together with Piezo ( Fig. 6 ). This combination should be implemented progressively along the specific steps of surgery. As a general principle, burrs should be used for reshaping bone, that is, for surface modifications, while Piezo should be employed for cutting bone, for which use it is unsurpassable. Likewise, Piezo is equally irreplaceable in posterior septoplasty when managing bony septal deviations and is highly effective for turbinoplasty. Regarding burrs, although the most popular are the spherical diamond burrs, those serve well to bevel bony edges but likewise tend to create grooves and thus cause potential irregularity of contour. This is why cylindrical, conical, and reversed conical burrs which have a flat surface, are ideal for reshaping the bone uniformly along a vast surface. This does not mean that power tools cannot also be used for cutting bone, which they obviously can, but the issue remains of avoiding periosteum injury, which is a huge advantage of using Piezo. These concepts are detailed in our recent publication, which highlights where and when to use Piezo and power in the standard modified dorsal split preservation hybrid primary rhinoplasty. However, even in those patients in which we follow a purely structural approach, Piezo and power are similarly blended together.
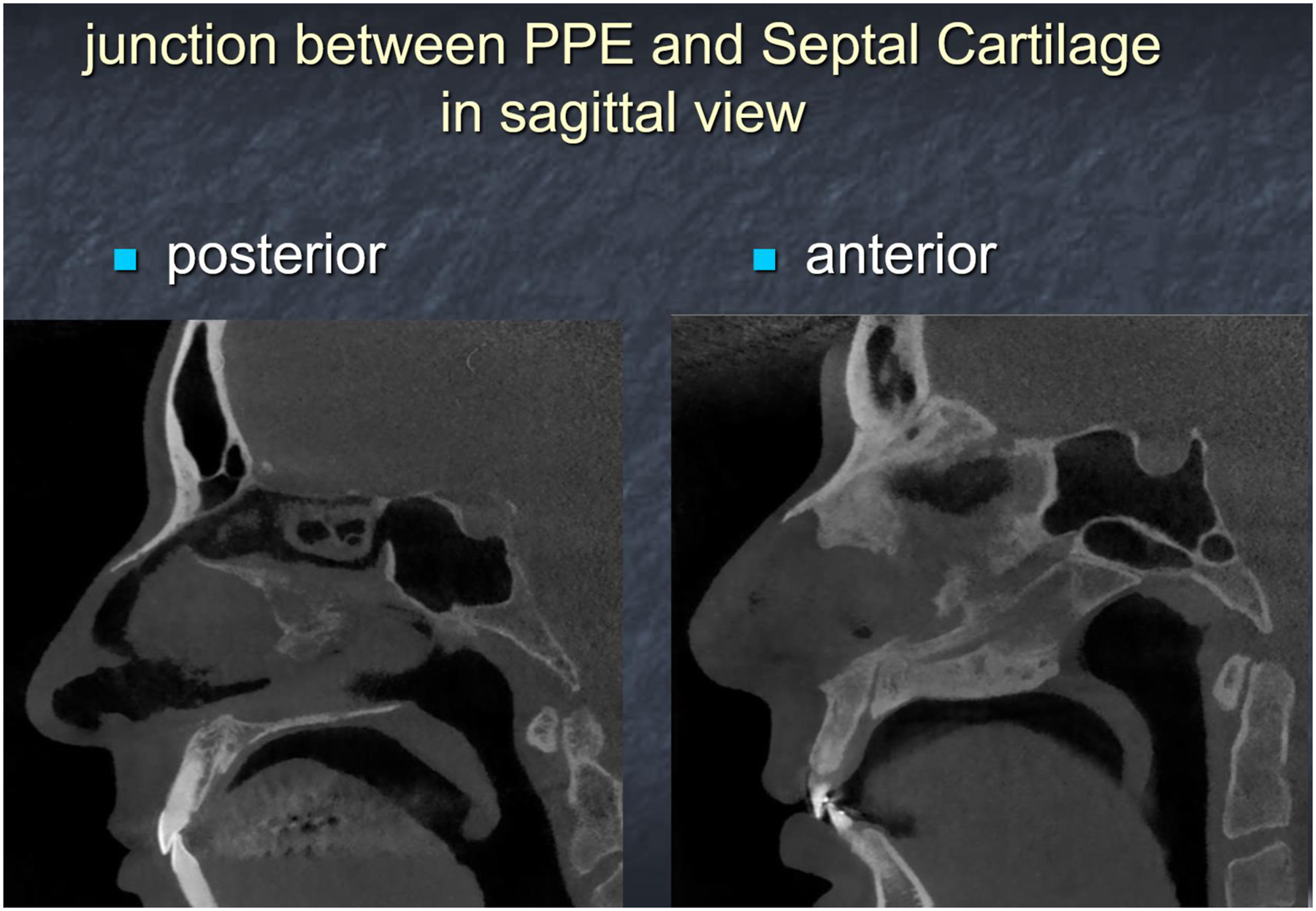
The Use of Cone Beam Computerized Tomography Scan and the Decision Process
A recurrent concept in this paper and our practice is that contemporary rhinoplasty is articulated and its algorithms diverse and still evolving. A standard rhinoplasty with its standard approach and standard techniques is a thing of the past. For this reason, it thus becomes logical that a diagnostic tool that can help the decision process and provide relevant information preoperatively is important, on condition that it is affordable in cost, practical, and fast to use. This is the case of the cone beam CT scan (CBCT), which we employ in 100% of our cases. A CBCT is a guiding tool with multiple applications in rhinoplasty as related to previewing anatomy in detail. , What essentially matters in favoring a preservation over a structural procedure, including the hybrid variations, is analyzing preoperatively: (1) the composition of the hump, whether cartilaginous or bony, and in which proportions, its height and length, also related to the V or S-shaped morphology; (2) the shape, symmetry, inclination, and thickness of the nasal bones; (3) the underlying extension of the upper lateral cartilages; and (4) the position of the perpendicular ethmoid plate junction as referred to the rhinion ( Figs. 7–9 ). This comes in conjunction with the traditional advantages of using a CT or CBCT in rhinoplasty, including evaluating the septum, the lower and middle turbinates, the nasal valves, the sinuses, as well as other elements like the thickness of the skin, the likely presence of fillers, and a wealth of additional information in secondary patients. Finally, the 3D reconstruction that provides clear imaging to highlight bone versus soft tissue provides a significant additional advantage with a CBCT. The intricacies of the shape and length of the nasal bones are well elucidated in the 3D view, together with the way they are reflected on the surface. It is striking how studying a CBCT image beforehand in a few minutes will already orient the decisional process, for instance between a cartilaginous pushdown (in a predominantly cartilaginous hump with a short bony cap) or a full letdown (in a V-shaped longer bony cap). Likewise, it may already orient toward the need for an osteoplasty in an S-shaped bony cap to be converted to a V-shape, toward an asymmetric letdown (in a longer and oblique nasal bone as compared to its more verticalized and shorter counterpart), or toward choosing the structural option for deformities best managed structurally. In essence, the use of the CBCT is a roadmap in all our rhinoplasties today. It is rapidly done, affordable, and with little inconvenience to the patient, with far less radiation exposure than conventional CT. The analysis is immediate, fast, and easy ( Box 1 ).
The initial steps
- 1.
Open approach via inverted-V incision
- 2.
Supraperichondrial dissection on the lower lateral cartilages and then transitioning to subperichondrial at the level of the scroll cartilages.
- 3.
Middle vault dorsal split along the septal T anatomic border (can be limited or occasionally avoided depending on the aesthetics of the dorsal lines. In such rare cases, a LKA release, in part or full, will then be necessary).
- 4.
Decision on a cartilaginous pushdown or a full letdown (planned preop but confirmed or modified intraop)
- 1.
- a.
Modified dorsal split cartilaginous push-down
- 1.
Bony cap initial reduction by Piezo or flat Burr and other osteoplasty (flat Burrs)
- 2.
High-middle septal strip excision proximal to the W point
- 3.
Lowering of the dorsum based on the elastic chondro-osseous joint at the K area (a notable variation here is possible, including a portion of the bony cap into the pushed-down DKA segment: the FurtadoKhazaal modification).
- 4.
L-strut septoplasty—piezo-assisted management of bony septal deviations
- 5.
Piezo-assisted turbinoplasty if needed
- 6.
Flexing the chondro-osseous junction by vertical incisions if needed
- 7.
Fixation by direct suturing, end-to-end or overlapping end-to-side
- 8.
Trimming the excess of upper lateral cartilages directly without LKA release (save the exception—in step 3—of a middle vault which is aesthetically acceptable: here, no split or partial split, partial or full lateral keystone (LKA) release, and suturing of the pushed down middle vault).
- 9.
Finessing the symmetry of the middle vault by spreader/spreaders if needed
- 10.
Resuturing the middle vault along the septal T anatomic border
- 11.
Conventional osteotomies/osteoplasty as needed—possible bone fixation by transcutaneous transosseous cerclage sutures
- 12.
Final osteoplasty if needed (burrs), including at the edges of the osteotomy sites
- 1.
- b.
Modified dorsal split full let-down
- 1.
Bony cap initial reduction by Piezo or flat Burr and other osteoplasty (flat Burrs)
- 2.
High-middle septal strip excision proximal to the W point
- 3.
Circumferential piezo osteotomies (symmetric or asymmetric letdown) (piezo and disc butt for transverse osteotomy)
- 4.
Dorsal lowering (checking potential blocking points)
- 5.
L-strut septoplasty—piezo-assisted management of bony septal deviations
- 6.
Piezo -assisted turbinoplasty if needed
- 7.
Flexing further the chondro-osseous junction by vertical incisions if needed
- 8.
Final osteoplasty if needed (burrs), including at the edges of the osteotomy sites
- 9.
Fixation by direct suturing, end-to-end or overlapping end-to-side
- 10.
Trimming the excess of upper lateral cartilages directly without LKA release (save the exception—in step 3—of a middle vault which is aesthetically acceptable: here, no split or partial split, partial or full LKA release, and suturing of the pushed down middle vault)
- 11.
Finessing the symmetry of the middle vault by spreader/spreaders if needed
- 12.
Resuturing the middle vault along the septal T anatomic border
- 1.
The final steps
- •
Structural tip plasty (usually small septal extension graft—currently “fusion sling” [Neves])
- •
Soft tissue redraping with 3-point compartmentalization technique and supratip break definition
- •
Skin closure
- •
Advantages and Disadvantages
Shortly said, regarding the modified dorsal split cartilaginous pushdown or full letdown techniques, the greatest advantages are predictability and full control. The open approach constantly allows full vision and is almost always followed by full dissection of the dorsum, which we find necessary since very few would be the patients in which the dorsum could be left completely undissected and undisturbed. Even in these instances, we prefer full exposure by complete degloving of the dorsum. Having said this, we recognize that other eminent colleagues will have excellent results in a closed approach and limiting or excluding dorsal dissection. Possibly, our patient population may be different, or simply we don’t wish to renounce to our open approach and structural background.
The main disadvantage is splitting the middle vault, which, in the “purist” preservation thinking would negate including the modified dorsal approach among preservation techniques for the very fact that the middle vault is opened. This strict point of view is obviously reasonable, but on the other hand this is why we call our technique hybrid with good reason. The middle vault is opened on an anatomic plane which is readily apparent when dissecting a nose, and the same junction between the edge of the septal T and the upper lateral cartilages can be easily reconstituted by a few sutures.
Regarding the hybrid instrumentation, the advantages have been detailed above, and will be readily obvious to anyone carefully comparing Piezo with Power and understanding what works better and in which circumstances. The main disadvantage here represents the cost and the availability of such instruments.
Practical Considerations and Anticipated Questions
- •
Is splitting the middle vault always necessary? No. It depends on the aesthetics and symmetry of the middle vault. The split can be partial or none, but then an LKA release (“ballerina maneuver” as defined by Goksel) is used. However, current dorsal preservation hybrid approaches do not necessarily imply faithfully preserving the full integrity of the dorsum.
- •
Why do we use a high-middle strip? . At the beginning of our experience, we were using a high strip and leaving the vertical stump of the septum attached to the septal T essentially too short, which made suture fixation difficult. Since we turned to a slightly lower strip, we derived 2 advantages: (a) a better suture fixation under direct vision, (b) some extra support of the horizontal septal L strut, when we overlap the septal T to whatever side is best indicated, which is something we do frequently. Also, importantly, the native residual septum is left high distally, which will leave a critical caudal septal support and avoid unwanted collapse at the supratip. What also matters, even regarding the learning curve, is that the septal L strut concept, so crucial in structural rhinoplasty, is not forgone. This is why, when possible, we prefer the high-middle strip to the low strip, also considering that we can harvest some cartilage more predictably. Maintaining the tenet of the L-strut principle will facilitate the transition to hybrid preservation techniques from the structural approach
- •
What about the blocking points? Those are well described in other key papers , and need to be well addressed to prevent inadequate lowering of the dorsum and a spring-back of the hump. This happened to me, especially in the beginning of my learning curve. What we find especially crucial is the dissection of perichondrium at the lateral osteotomy as well as the excision of a triangle of bone (the “banana” takeout as defined by Haack), so as to allow the proper vector of lowering-rotation of the dorsum.
- •
Is there a bailout option? Yes. A bridge is still open, once the middle vault is split, to convert to a component separation—incremental reduction structural concept. This could be especially useful when, for whatever reason, the DKA detaches fully from the remaining dorsum. However, while a cartilaginous push-down can still be converted to a full structural at any time, the red line crossing after which no going back is possible in a full let-down is once the circumferential osteotomy has been completed.
- •
What about the tip? The tip is constantly done structural, on a supra-perichondrial plane, dissection being carried out with the 3 points compartmentalization technique. My preference is to change the plane from supraperichondrial to subperichondrial at the vertical scroll area. We have embraced the concept of the sub-laminar rather than subperichondrial septal dissection, as well as the use of the “septal fusion” sling as well described by Neves. , This has superseded for us the use of the interdomal ligament for supporting the tip, as we were doing previously, although without having ever published this method. A properly designed and shaped septal extension graft is used in most instances, and a small strut is always added essentially as a spacer graft. Maximum control of the dead space is achieved by side wall laminas, as well as by Doyle splints. Recently, we have gathered some experience with the use of transcutaneous sutures as described by Zholtikov in thick and/or loose-skinned patients. It is too early to state that this has a related advantage in our practice, but we can surely state that if carefully done, transcutaneous suturing will leave no permanent marks.
Summary
Finding The Way in the maze of contemporary rhinoplasty techniques is definitely not easy. The spectrum of options is becoming so articulated that beginners have difficulty in understanding which technique to follow, while experienced surgeons are faced with the dilemma of exploring unfamiliar grounds. Even in this case, one essentially has to choose between the intriguing perspective of further improving one’s results or taking the reassuring decision to forego and stay with what one is confident with. My current conclusion, after a few years of rather obstinately dealing with new concepts and new techniques, is that the hybrid concepts detailed above probably represent the best of the two worlds. I can now say that the results have made this journey worthwhile.
Clinical case
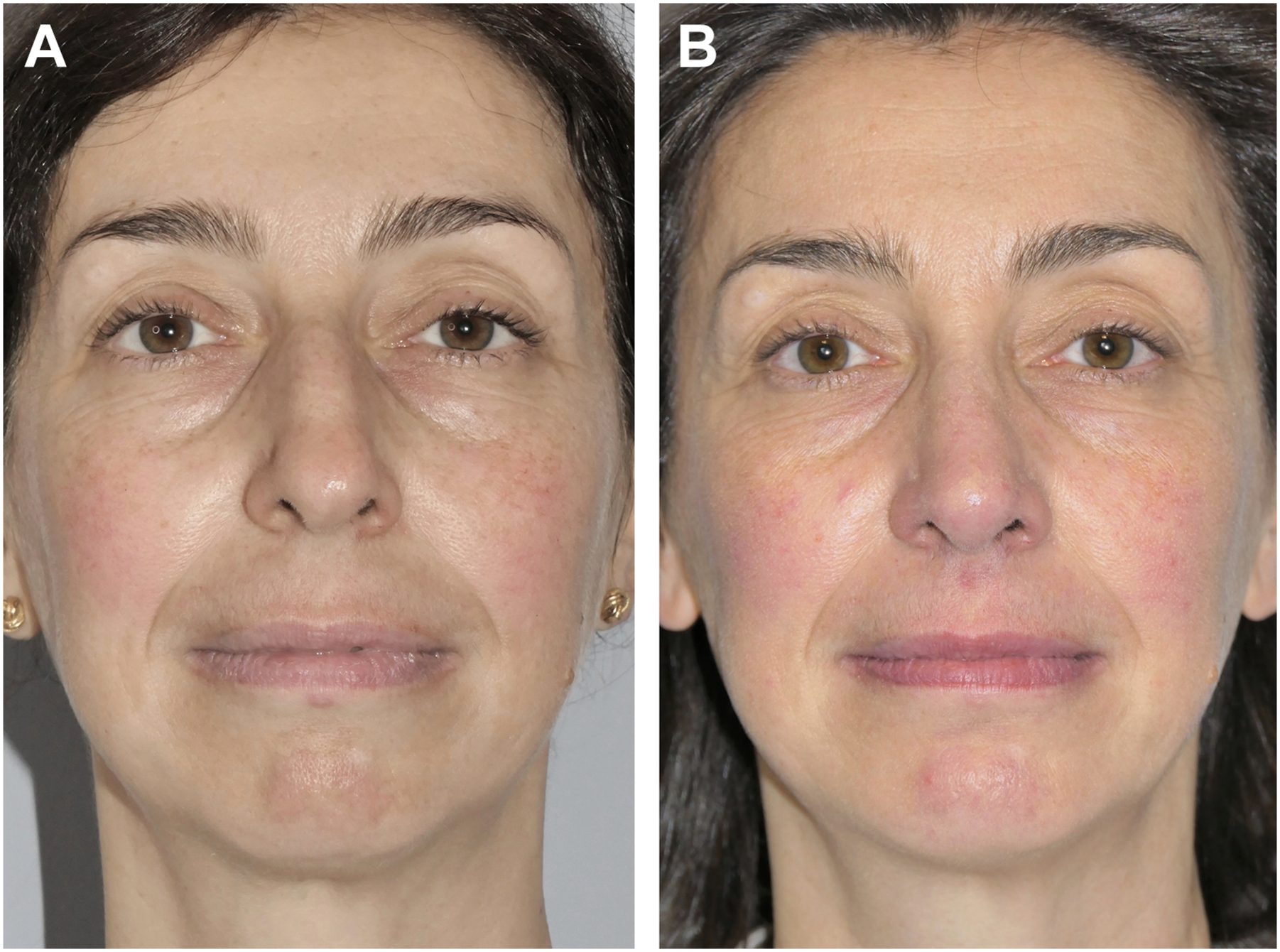
This 46-year-old patient underwent an open approach with full letdown following subperichondrial subperiosteal elevation of the skin envelope, split of the middle vault, and a high middle strip resection with right side overlap. Osteoplasty was done by burrs and circumferential osteotomy by Piezo, save for the transverse osteotomy done by disc burr. Structural techniques were used for the tip, including multiple tip sutures, slide under of the upper border of the lower laterals, a small septal extension graft in end-to-side to the distal septum, interdomal ligament sling, and 3 point dorsum compartmentalization. A silicone anatomic implant was inserted via an endo-oral incision ( Figs. 10A–15 B ). Preoperative and 9 months postoperative views are depicted in Figs. 1–6 . In Figs. 7 and 8 , the CBCT scan demonstrates a rather long and tall bony cap, which can be brought to a V-shape, ideal for letdown purposes, by osteoplasty (see figures captions).
Related posts:
 Understanding Dorsal Preservation Rhinoplasty
Understanding Dorsal Preservation Rhinoplasty
 Alar Preservation Principles
Alar Preservation Principles
 ischemia in microvascular breast reconstruction
for lymphedema: clinical research and long-term results
Invasive Component Separation Results in Fewer Wound-Healing Complications than Open Component Separation for Large Ventral Hernia Repairs
ischemia in microvascular breast reconstruction
for lymphedema: clinical research and long-term results
Invasive Component Separation Results in Fewer Wound-Healing Complications than Open Component Separation for Large Ventral Hernia Repairs
 Hand and Wrist Anatomy and Examination
Hand and Wrist Anatomy and Examination
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


