38 Holding Solutions
Summary
Keywords: HypoThermosol ATP holding solution cold injury ischemia reperfusion injury normal saline
Key Points
•There are two different categories of holding solutions: intracellular and extracellular.
•Extracellular solutions include intravenous (IV) rehydration fluids (saline, lactated ringers) and culture media. These are not designed to protect tissue during chilled storage conditions.
•Intracellular solutions include tissue preservation solutions, which have been especially designed to hold tissue during chilled storage conditions; HypoThermosol/adenosine triphosphate (ATP) is an example.
•There are no high-quality studies comparing graft holding solutions for hair transplantation. Small extended storage studies are particularly helpful in this area.
38.1 Introduction
When hair transplantation consisted of moving smaller numbers of larger grafts, the “out-of-body” time for tissue was relatively short. Consequently, simple hydration with normal saline was considered adequate to protect tissue. As cases became longer, tissue “storage” became a much more important issue given that time out of body could last anywhere from 2 hours to over 12 hours. Because of conflicting data about which storage solution is best, most surgeons have continued to use normal saline, but there are a variety of other solutions that are in use today. Table 38.1 lists several of the holding solutions that have been reported for use during hair transplantation. It is important to note that none of these have achieved any regulatory approval as a hair follicle holding solution during hair transplantation. The diversity of practices and lack of consensus regarding which solution is optimal reflects the complexity of this topic.
The issue of holding solutions for hair follicle grafts must be considered within the overall framework of graft survival. The reader is referred to Chapter 5 for a review of all the factors related to graft survival. Assuming the surgeon wishes to achieve the highest possible graft survival in every patient, holding solutions can be viewed as one component of a coordinated protocol spanning donor harvesting, graft preparation and implantation, and ending with oxygenation and revascularization of the grafts. Simply using a new and better holding solution before mastering basic surgical techniques, which are the foundation of excellent graft survival, is unlikely to be fruitful; for example, there is widespread consensus that follicle trauma (transection, dehydration, crushing) is the most important obstacle to graft survival. Even if a “perfect” holding solution were identified, it would be of little value if excellent surgical technique were not employed to prevent follicle trauma. Holding solutions will not correct for poor technique.
For the surgeon interested in studying holding solutions for hair transplantation, two important observations are worth considering:
•Experts in the field of organ transplantation cannot agree on the best organ preservation holding solution. There is ongoing research and much disagreement as to which solution is superior for keeping organs such as livers, kidneys, and hearts viable while outside the body prior to transplantation. There is active research and new products are under development. We should therefore expect that defining the optimal hair transplant holding solution would be complicated and full of uncertainty as well.
•Normal saline has been used for many decades as a holding solution for hair transplants and is generally considered to be satisfactory. There are many reasons why saline should be a poor choice as a holding solution (discussed later) and yet it appears to produce acceptable results. This should clarify that overall the role of holding solutions in effecting graft survival is not as great as follicle trauma or graft oxygenation.
To understand the role of time out of body on grafts, Limmer studied the survival of follicular unit grafts stored in chilled saline for various time periods prior to implantation.1 Not unexpectedly, there was a time-dependent decrease in graft survival for grafts stored outside the body between 2 and 48 hours prior to implantation (Fig. 38.1). Subsequently, Kim and Hwang replicated these results and also showed that chilling appears to have little benefit for shorter storage times (<4 hours outside of the body) compared to room temperature storage.2 Given that most modern procedures may involve keeping grafts out of body for 2 to 12 hours, one might predict 85 to 95% survival when chilled saline is used based on Limmer’s results. However, it is important to keep in mind that only small study boxes containing a limited number of grafts were used. In actual practice, the range in graft survival is much wider. Assuming that experienced surgeons may routinely achieve approximately 90% graft survival, the theoretical benefit of an optimized holding solution may be in the range of 5 to 10%. Whether such a benefit is worthwhile may depend on the cost of these alternative holding solutions. Besides an improvement in overall graft survival, improved holding solutions may also result in grafted hair that is more robust and grows in sooner after surgery.
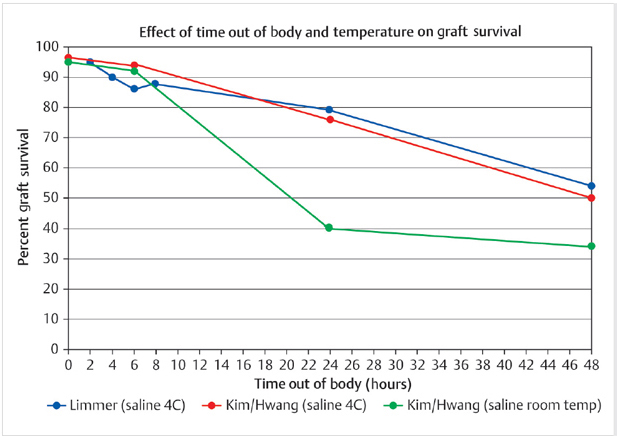
Fig. 38.1 Graph demonstrating survival of grafts stored long-term in saline either chilled or at room temperature. Because of the small number of subjects studied, the exact percentage of survival is not generalizable, but the decrease in survival over time is obvious. These studies suggest, but do not prove, that chilling may not be necessary for short storage times.
With this in mind, the author tested HypoThermosol FRS (BioLife Solutions, Bothell, Washington, United States), both with and without the addition of the liposomal adenosine triphosphate (ATP; ATPv, Energy Delivery Solutions, Jeffersonville, Indiana, United States) during an extended storage study.3 The patient was a 70-year-old man who had recently had a skin cancer excised, followed by a course of radiation therapy on his left temple. This left a large area of complete alopecia in the area. We first excised the donor strip on day 1, and dissected the follicular unit grafts under the microscope. We then divided the grafts into three groups: (1) HypoThermosol + liposomal ATP, (2) HypoThermosol without ATP, and (3) saline; the grafts were stored in these solutions for 5 days at 4°C, after which they were placed into the scalp using standard technique. In addition, all of the areas were sprayed postoperatively with liposomal ATP, so the only difference between the three groups was the storage solutions used.
The patient was followed periodically and final hair counts and photographs were performed at 18 months. Graft survival per area was (1) 72% for HypoThermosol/ATP, (2) 44% for HypoThermosol alone, and (3) 0% in saline. HypoThermosol with liposomal ATP was the clear winner (Fig. 38.2). Whereas this study was only of a single patient, it is the longest survival study of hair grafts ever reported (to the author’s knowledge). And it does suggest that there would be some benefit even during shorter storage times (e.g., 2–6 hours) of a standard hair transplant. This study was corroborated when Michael Beehner subsequently reported that much smaller graft totals but at more frequent intervals (2–96 hours) also showed significantly better results for HypoThermosol + ATP compared to saline.4 In his study, use of this holding solution resulted in not only greater survival but also more robust hair shafts using a graded scoring system for hair caliber.

Fig. 38.2 (a,b) Eighteen months following transplantation of grafts stored for 5 days at 4°C in HypoThermosol/adenosine triphosphate (ATP).
Related posts:
 Methods and Techniques to Study Hair Cell Survival
Methods and Techniques to Study Hair Cell Survival
 The Patient with Minimal Hair Loss: Planning and Decision-Making
The Patient with Minimal Hair Loss: Planning and Decision-Making
 The Young Patient: Planning and Decision-Making
The Young Patient: Planning and Decision-Making
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 East,West, and Southern Asian Hair Transplant Specifics
Contact Management Software and Its Utilization as a Marketing Tool
East,West, and Southern Asian Hair Transplant Specifics
Contact Management Software and Its Utilization as a Marketing Tool
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


