Fig. 16.1
Diagram over a normal epidermis showing the location of the microscopic vesicles in the different autoimmune blistering diseases (hematoxylin-eosin stain; original magnification ×200)
16.1.1 Intraepidermal Blistering Diseases
16.1.1.1 Pemphigus Vulgaris
The initial histological finding in pemphigus vulgaris (PV) is the appearance of intercellular edema between keratinocytes that ultimately leads to a separation between cells and rupture of the spinous processes leading to a phenomenon that we call acantholysis. In PV this process takes place characteristically in the suprabasal layer, producing suprabasal intraepidermal blisters, and there may be cells floating inside the vesicle, the so-called acantholytic cells. These cells are round, with a hyperchromatic nucleus and homogeneous cytoplasm. The cells of the basal layer remain attached to the basement membrane zone (BMZ) by their hemidesmosomal attachments and produce a characteristic image that has been compared to a row of tombstones (Fig. 16.2a) [1]. In the underlying dermis there are usually mild to scarce perivascular inflammatory infiltrates of mononuclear cells and some eosinophils. In some cases the epidermal changes are absent, and acantholysis can only be seen in the follicular epithelium selectively, without affecting the interfollicular epidermis [2]. In some patients, before blistering occurs the patients present with inflammatory plaques that show histologically a spongiotic dermatitis with abundant eosinophils within the epidermis, a histological pattern that has been referred to as eosinophilic spongiosis [3]. Although this finding was initially described in pemphigus (both vulgaris and foliaceus), it can be seen in other autoimmune bullous diseases and in other disorders. In fact, eosinophilic spongiosis is much more frequently seen in the pre-bullous stages of bullous pemphigoid than in pemphigus.
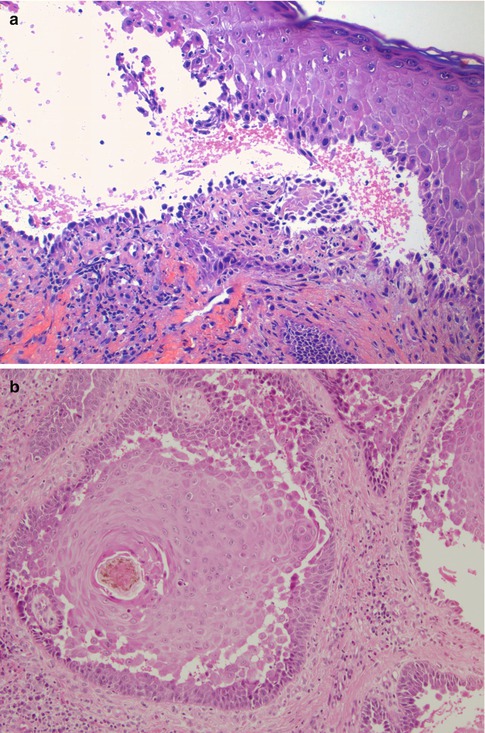
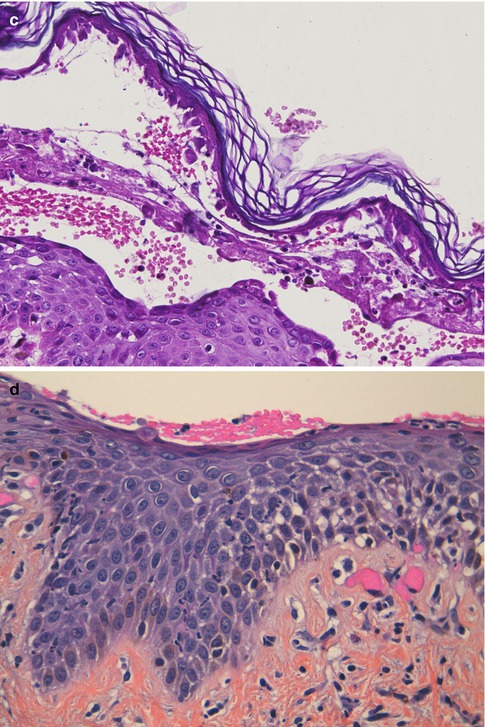
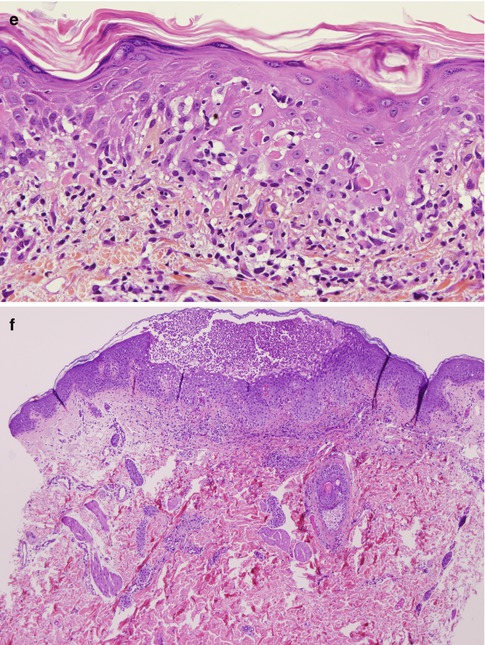
Fig. 16.2
(a) Pemphigus vulgaris. Intraepidermal blister located suprabasally with acantholytic cells floating inside the vesicle. The cells of the basal layer remain attached to the basement membrane zone showing a characteristic row of tombstone pattern (hematoxylin-eosin stain; original magnification ×200). (b) Pemphigus vegetans. Acanthosis and pseudoepitheliomatous hyperplasia together with suprabasal clefting and prominent acantholysis (hematoxylin-eosin stain; original magnification ×100). (c) Pemphigus foliaceus. Intraepidermal blister located within the stratum corneum (subcorneal) with some acantholytic cells floating inside the vesicle (hematoxylin-eosin stain; original magnification ×200). (d) Pemphigus foliaceus. There is no evident intraepidermal blister. The clues for diagnosis are the absence of stratum corneum and granulosum and the presence of neutrophilic spongiosis (epidermal spongiosis with presence of neutrophils) (hematoxylin-eosin stain; original magnification ×200). (e) Paraneoplastic pemphigus. There is no acantholysis. The biopsy shows a prominent lichenoid dermatitis with several necrotic keratinocytes and basement membrane vacuolization. This patient had an associated follicle center lymphoma (hematoxylin-eosin stain; original magnification ×200). (f) IgA pemphigus of the subcorneal pustular dermatosis subtype. Subcorneal pustule with abundant neutrophils and superficial epidermal spongiosis (hematoxylin-eosin stain; original magnification ×40)
The findings in pemphigus vegetans (PVeg) show some characteristics that are different from those of PV. Although early lesions may show suprabasal acantholysis, as in PV, fully developed lesions of PVeg will show acanthosis and papillomatosis, sometimes with prominent pseudoepitheliomatous hyperplasia, and the presence of intraepidermal abscesses of eosinophils. Suprabasal acantholysis may be very subtle and therefore may be missed in some cases (Fig. 16.2b) [4]. The differential diagnosis has to be done with conditions like pyostomatitis vegetans, Hailey-Hailey disease, or blastomycosis-like pyoderma (also known as pyoderma vegetans). Classically, PVeg can be divided in two subtypes, the Neumann and the Hallopeau subtype, that differ clinically and histologically. In the Neumann subtype, lesions are characterized by papillomatosis and acanthosis with intraepidermal vesiculation and suprabasal acantholysis. Intraepidermal pustules of neutrophils and eosinophils are scant or absent. In the Hallopeau subtype, lesions will also demonstrate acanthosis with occasional acantholysis, but with numerous and large eosinophilic abscesses, as well as areas of eosinophilic spongiosis. In late lesions the histological findings will overlap in both subtypes.
16.1.1.2 Pemphigus Foliaceus and Erythematosus
The histopathological findings in endemic and non-endemic pemphigus foliaceus (PF), pemphigus erythematosus, and drug-induced cases of pemphigus are identical. They are characterized by the presence of superficial acantholysis, just below the granular layer of the epidermis (Fig. 16.2c). Initial vesicles can contain abundant neutrophils or eosinophils. Occasionally, as a result of the blisters having a very thin ceiling, they break and loose the upper layer. This may give the appearance of a “normal epidermis” or even of a psoriasiform dermatitis, with no clear finding of acantholysis. The clue for diagnosis in these cases is the absence of stratum corneum and parts of the stratum granulosum (Fig. 16.2d) [5]. The main differential diagnosis here is with impetigo and staphylococcal scalded skin syndrome that are both disorders caused by the cleavage of the extracellular domain of desmoglein 1 by a toxin produced by certain strains of Staphylococcus aureus.
The pattern of eosinophilic spongiosis can also be seen as an initial feature in PF and is also the typical histological pattern of pemphigus herpetiformis that often evolves to PF [3, 6]. Another pattern that may be observed in early lesions of pemphigus (particularly in PF) is that of neutrophilic spongiosis [7].
16.1.1.3 Paraneoplastic Pemphigus
The classic pattern described in paraneoplastic pemphigus (PNP) is the presence of intraepidermal blisters with suprabasal acantholysis (similar to PV), combined with lichenoid changes including interphase dermatitis, presence of necrotic keratinocytes and lichenoid inflammatory infiltrates [8]. These histological findings are not completely specific of PNP and they have also been found in erythema multiforme, toxic epidermal necrolysis, and approximately one third of cases with other forms of pemphigus [9]. In the personal experience of the author, the classic pattern of PNP can be observed in only 20 % of the biopsies from these patients, while 50 % of the biopsies showed a histological pattern indistinguishable from PV (intraepidermal blisters with suprabasal acantholysis), and 30 % of the biopsies showed only purely lichenoid changes without acantholysis (Fig. 16.2e). Sometimes we can observe the combination of the different patterns in different biopsies (i.e., one biopsy showing suprabasal acantholysis and another a lichenoid pattern). Eosinophilic spongiosis has also been reported in PNP [10].
16.1.1.4 IgA Pemphigus
There are two major clinicopathological subtypes of IgA pemphigus (IAP). In the subcorneal pustular dermatosis subtype of IAP, histological examination of the lesions shows epidermal spongiosis with exocytosis of neutrophils and some eosinophils and the formation of subcorneal collections of neutrophils (Fig. 16.2f). Acantholysis is usually not seen, and if it is present, there are usually only isolated cells. In the superficial dermis there are perivascular infiltrates of neutrophils, eosinophils, and lymphocytes [11]. The differential diagnosis in this subtype of IAP must be made with subcorneal pustular dermatosis of Sneddon-Wilkinson, pustular psoriasis, acute generalized exanthematous pustulosis, or impetigo. The intraepidermal neutrophilic dermatosis subtype of IAP shows epidermal acanthosis with spongiosis and exocytosis of neutrophils and eosinophils. These cells tend to form microabscesses and pustules inside the stratum spinosum of the epidermis. In the dermis there is papillary edema and perivascular infiltrates with abundant neutrophils, eosinophils, and lymphocytes. Acantholysis is also very rare in the biopsies of these patients, although some cases have been reported where there were suprabasal blisters identical to those of PV [12, 13]. The differential diagnosis in this subtype of IAP has to be done with pemphigus vegetans (Hallopeau type) and halogenodermas. Patients with IAP with features of PV or PF have also rarely been reported, and they were histologically identical to conventional PV or PF.
16.1.2 Subepidermal Blistering Diseases
16.1.2.1 Bullous Pemphigoid
Histopathological examination of the vesicles and blisters of bullous pemphigoid (BP) demonstrates subepidermal blisters with abundant eosinophils and variable amount of lymphocytes and macrophages in the superficial dermis [14]. The inflammatory cells are distributed within the subepidermal blister and around the vessels of the superficial vessels (Fig. 16.3a). It is unusual to observe the presence of inflammatory cells in the mid- or deeper dermis, and its presence may favor other entities such as arthropod bite reactions, bullous drug reactions, eosinophilic dermatosis associated with hematologic malignancies, or Wells’ syndrome. When the biopsy has been taken from an old lesion, the histological findings may be those of an intraepidermal blister, due to reepithelialization of the blister floor, and this may lead to confusion with pemphigus. Sometimes in evolved lesions instead, there may be necrosis of the epidermal roof of the blister, leading to confusion with other blistering diseases like erythema multiforme or toxic epidermal necrolysis.
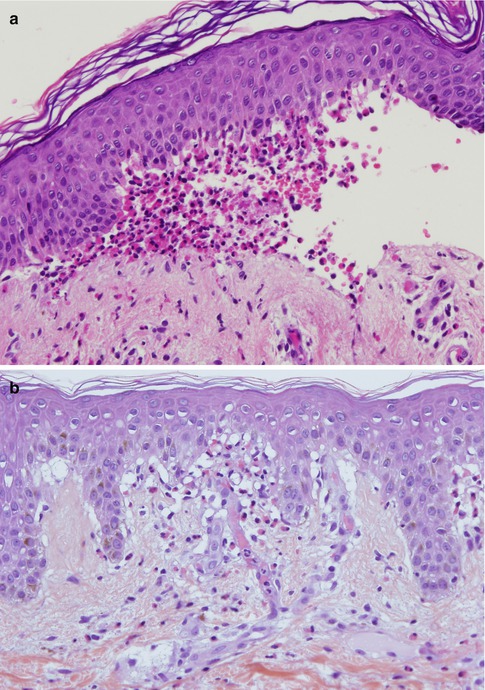
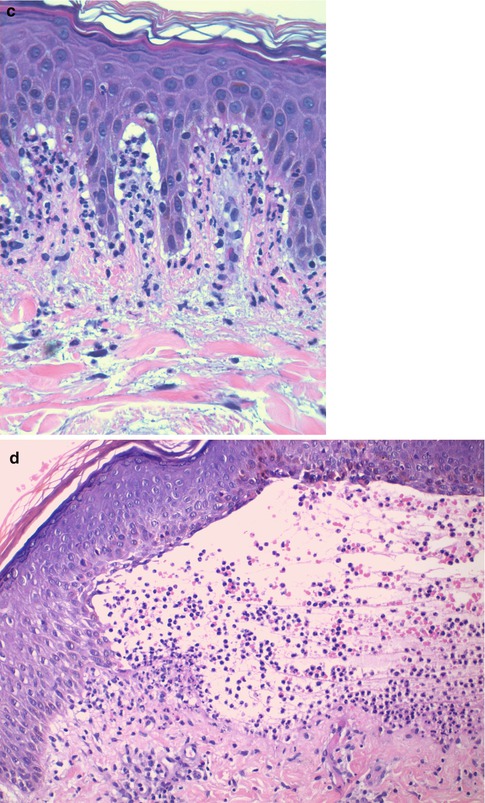
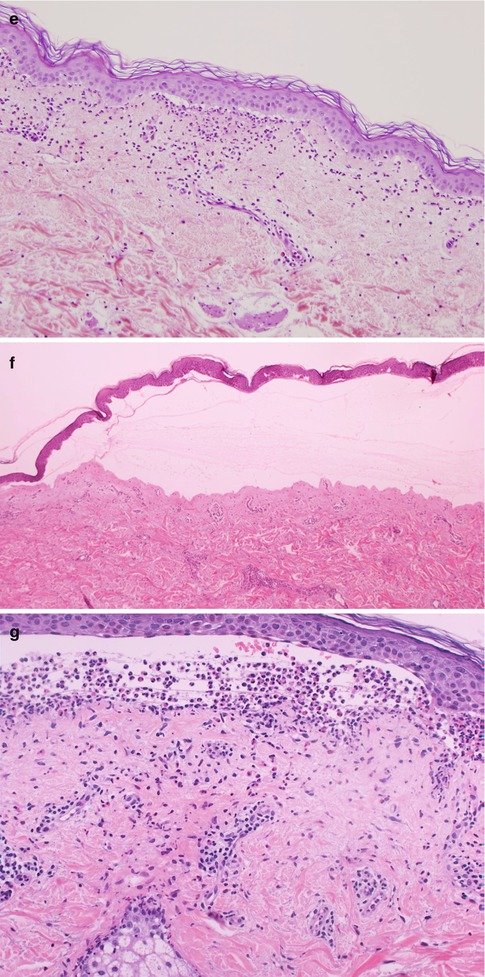
Fig. 16.3
(a) Bullous pemphigoid. Subepidermal blister with abundant eosinophils within the vesicle and in the superficial dermis (hematoxylin-eosin stain; original magnification ×200). (b) Eosinophilic spongiosis. Epidermal spongiosis with the presence of eosinophils. This pattern is not specific for pemphigoid, as it can be observed in other immunobullous disorders, as well as in other inflammatory conditions (hematoxylin-eosin stain; original magnification ×200). (c) Dermatitis herpetiformis. Characteristic microabscesses of neutrophils at the tips of the dermal papillae (hematoxylin-eosin stain; original magnification ×400). (d) Dermatitis herpetiformis. Subepidermal vesicle with superficial inflammatory infiltrates with abundant neutrophils and the presence of scattered eosinophils (hematoxylin-eosin stain; original magnification ×200). (e) Linear IgA bullous dermatosis. Neutrophils aligning along the basement membrane zone at the edges of a subepidermal blister with abundant neutrophils (not shown in the picture). There is also an associated basal vacuolization (hematoxylin-eosin stain; original magnification ×100). (f) Epidermolysis bullosa acquisita, mechanobullous subtype. Subepidermal blister with nearly absent inflammation (there are scant perivascular lymphocytes) (hematoxylin-eosin stain; original magnification ×40). (g) Epidermolysis bullosa acquisita, inflammatory subtype. Subepidermal blister with abundant inflammatory infiltrates in the superficial dermis and within the blister where neutrophils predominate. There is also nuclear dust, abundant eosinophils, and neutrophils aligning along the basement membrane zone of a sebaceous gland in the deepest part of the biopsy (hematoxylin-eosin stain; original magnification ×200)
When urticarial or eczematous lesions are biopsied, as well as in the prodromal stages of BP (the so-called urticarial stage of BP), histological findings are less specific. The typical findings will be those of superficial perivascular dermatitis with abundant eosinophils and edema of the papillary dermis, and in some cases, in addition, eosinophilic spongiosis can be observed (Fig. 16.3b) [15]. In the author’s personal experience, the observation of eosinophilic spongiosis with eosinophils aligned along the BMZ in an elderly patient (older than 70 years) is highly predictable of BP.
16.1.2.2 Pemphigoid Gestationis
In pemphigoid gestationis (PG) the histopathological examination of lesional skin biopsies shows similar findings to those seen in BP. There is a subepidermal separation with inflammatory infiltrates rich in eosinophils, with lymphocytes and histiocytes both in the superficial dermis and within the blisters. When early/urticarial lesions are biopsied, there is dermal papillary edema, with superficial dermal inflammatory infiltrates with eosinophils, and occasionally eosinophilic spongiosis [16]. In these early lesions, the differential diagnosis with polymorphic eruption pregnancy can be very difficult based on histology alone. Both direct immunofluorescence and serologic testing will be needed [17].
16.1.2.3 Mucous Membrane Pemphigoid
Histological examination is presently not considered as an absolute criterion for the diagnosis of mucous membrane pemphigoid (MMP). At an international consensus held in Chicago in 1999, a group of experts concluded that biopsies of a blister (especially from the eye) or demonstration of a subepithelial blister was not always possible, and therefore, the participants did not consider results from light microscopic studies as an absolute criterion for diagnosis [18]. When the skin is affected, the biopsy should be performed from the skin. When there are multiple affected mucosae (but not the skin), the oral mucosa should be biopsied. If there is only involvement of one mucosa (such as the eye or others), then the biopsy has to be done from this location [19], but in all cases direct immunofluorescence (DIF) examination is of priority. When histological studies of a lesion are available, they can demonstrate subepithelial blisters with moderate superficial inflammatory infiltrates that can be varied in cell type, but usually plasma cells and lymphocytes predominate. Although these findings are different to the ones that we would expect in other disorders such as erosive lichen planus (which should show lichenoid infiltrates, basement membrane vacuolization, and necrotic keratinocytes), there is often a histological overlap between MMP and erosive lichen planus, and therefore, DIF examination is key to the diagnosis.
16.1.2.4 Dermatitis Herpetiformis
The classic histopathological findings in dermatitis herpetiformis (DH) are well known, but cannot be considered specific to this entity. In the initial stages, biopsies show the characteristic pattern of microabscesses of neutrophils at the tips of the dermal papillae with fibrin deposits (Fig. 16.3c). As the lesions evolve, subepidermal vesicles with superficial inflammatory infiltrates (both in the dermis and in the blister) composed of lymphocytes, histiocytes, eosinophils, and abundant neutrophils with nuclear dust can be observed. In these lesions we may observe neutrophilic papillary microabscesses at the edges of the blisters (Fig. 16.3d). However, sometimes the pathological findings are not typical. In evolved lesions the inflammatory infiltrates may show the presence of abundant eosinophils, resembling BP. Some authors have even described a pattern similar to arthropod bites with severe edema in the papillary dermis with a mixed infiltrate by multiple eosinophils and “flame figures” in the reticular dermis [20]. However, in the author’s experience, the most important problem in the histological diagnosis of DH is tissue sampling. Most patients present to the clinic with multiple excoriated lesions caused by scratching, but without any visible vesicle or blister. Therefore, in as much as half of the cases, the biopsy will show nonspecific findings such as spongiotic dermatitis, lichen simplex chronicus, changes of excoriation, prurigo nodularis-like lesions, or lymphocytic infiltrate only with fibrosis in the dermal papillae and ectatic capillaries [21].
16.1.2.5 Linear IgA Bullous Dermatosis
Linear IgA bullous dermatosis (LABD) is characterized by the presence of subepidermal vesicles and superficial inflammatory infiltrates containing abundant neutrophils both in the dermis and in the blister accompanied by a variable number of eosinophils and nuclear dust. These vesicles may be totally indistinguishable from the findings detected in DH. However, on the edges of the vesicle, neutrophils tend to be arranged along the BMZ, and this is associated with basal vacuolization (Fig. 16.3e). These findings are also not specific to LABD, as they can be also found in epidermolysis bullosa acquisita (EBA) and bullous systemic lupus erythematosus (BSLE), among others. In some cases neutrophils form microabscesses in the papillae, indistinguishable from those observed in DH. When comparing these two entities, the number of rete tips with neutrophils with basal vacuolization and the length of the BMZ associated with these findings were greater in LABD than DH, while the number of microabscesses of neutrophils in the dermal papillae was greater in DH than in LABD [22]. However, DIF examination must be done to clearly establish each of the above diagnoses with confidence.
16.1.2.6 Epidermolysis Bullosa Acquisita
Histological examination of lesional biopsies in EBA will show subepidermal blisters with variable inflammatory infiltrates depending on the disease phenotype [23]. In the classical mechanobullous phenotype of EBA, the inflammatory reaction is absent, or there are very few superficial perivascular infiltrates of lymphocytes (Fig. 16.3f). These findings may be similar to those observed in the inherited forms of epidermolysis bullosa or certain forms of porphyria. In the inflammatory phenotype of EBA, in contrast, there are abundant inflammatory infiltrates in the superficial dermis where neutrophils predominate [24]. Neutrophils aligned along the BMZ with basal vacuolization can also be seen both in the epidermis and the adnexal structures. Papillary microabscesses of neutrophils, nuclear dust, abundant eosinophils, and even eosinophilic spongiosis can also be seen, although less frequently (Fig. 16.3g). The differential diagnosis in these cases can be broad and has to be done with BP, MMP, DH, LABD, or BSLE. DIF examination will help to differentiate inflammatory EBA from DH or LABD. Recent studies suggest that the inflammatory phenotype of EBA is the most frequent phenotype (up to two thirds of the patients) [25], and therefore, additional studies will be needed to differentiate these patients from other patients with IgG-mediated subepidermal blistering diseases.
16.1.2.7 Bullous Systemic Lupus Erythematosus
In BSLE the histological findings will be identical to the inflammatory phenotype of EBA. Therefore, the biopsies will show the presence of subepidermal blisters with a neutrophilic infiltrate in upper dermis and/or papillary microabscesses of neutrophils [26–28]. In addition some patients may show basement membrane vacuolization and nuclear dust [29].
16.1.2.8 Other Autoimmune Subepidermal Blistering Diseases
Several new subepidermal blistering diseases have been described in the past two decades. The most frequent of these, even if they are rare, are anti-laminin-332 MMP and anti-p200 pemphigoid. In anti-laminin-332 MMP (also called anti-epiligrin cicatricial pemphigoid or anti-laminin-5 MMP), histological findings show a subepidermal blister with dermal inflammatory infiltrates of variable intensity where lymphocytes tend to be the predominant cell type seen; however, neutrophils and eosinophils can be observed in early lesions. In older lesions, a characteristic finding is lamellar fibrosis in the upper dermis. Mucosal lesions may have a lichenoid infiltrate in the upper submucosa very similar to erosive lichen planus [30, 31]. In anti-p200 pemphigoid, biopsies show subepidermal blisters with inflammatory infiltrates in the upper dermis that can be composed by mainly neutrophils or a mixed infiltrate with both neutrophils and eosinophils. Neutrophilic microabscesses, neutrophilic spongiosis, or eosinophilic spongiosis may also be observed [32]. Therefore, anti-p200 pemphigoid shows histological features that look like LABD, DH, or even BP.
16.2 Immunofluorescence Studies
16.2.1 Direct Immunofluorescence Staining
Direct immunofluorescence (DIF) is a technique placed between conventional histopathology and laboratory techniques. It was introduced in the field of dermatology in the early 1960s and up to now remains a very useful technique for the diagnosis of different inflammatory skin diseases, and it must be considered essential for the diagnosis of autoimmune blistering diseases. DIF is basically an immunohistological staining that allows the detection of the presence of antibodies or other proteins in skin biopsies of various skin conditions [33–35].
In general, a biopsy from patients with autoimmune blistering diseases must be taken from perilesional normal or erythematous skin (unlike other diseases like lupus erythematosus). Biopsies of vesicles or blisters should be avoided as they will often show false-negative results. Once the tissue has been obtained by punch or excision, the sample must be frozen immediately in liquid nitrogen or placed in saline for subsequent freezing after a short time. In those cases where the immunofluorescence laboratory is not found near the center where the biopsy is done, the tissue has to be placed in a transport medium. The most used by dermatologists is Michel’s medium, a solution that will preserve the biopsy for several days or even weeks at room temperature [36, 37]. The sample can then be sent by mail to the laboratory where it will be washed in Michel’s washing medium, frozen, and later processed for immunofluorescence. It has been recently observed that the best results are obtained if the biopsy is kept in saline for about 24 h (instead of directly freezing the biopsy) when the sample reaches the laboratory [38]. This procedure “washes away” the tissue and decreases the background staining. Those biopsies that will arrive to the laboratory after a longer period (more than 24 h) should be sent in Michel’s medium. Another concern that should be mentioned is that if a biopsy for DIF is accidentally immersed in formalin, this can cause both false-negative and false-positive findings that make them less suitable for the diagnosis, and therefore, taking a new biopsy would be advisable [39].
In the next steps, the biopsy is frozen (usually after inclusion in OCT), and 4–6 μ[mu]m section is obtained using a cryostat. Subsequently, the sections will be incubated with polyclonal antibodies directed against human IgG, IgA, IgM, C3 fraction of complement, and fibrinogen conjugated with fluorescein isothiocyanate (FITC). Finally, after washing the biopsy several times to remove the unbound antibodies, tissue sections are examined using a fluorescence microscope. The blue light (wavelength 488 nm) emitted from the light source is capable of exciting FITC, and this molecule will emit a wavelength of 520 nm that will be seen under the microscope with an apple green color.
16.2.1.1 Intraepidermal Blistering Diseases
Pemphigus Vulgaris
DIF of perilesional biopsies obtained from the skin or mucous membranes from PV patients will show the deposition of IgG on the cell surface of epidermal keratinocytes in almost all patients with active disease [40]. Although these deposits are usually found in all epidermal layers and in the adnexae (hair follicles and eccrine glands), in some patients these deposits are more intense or only found in the lower third of the epidermis (Fig. 16.4a, b). These deposits may be linear and intense and show a fishnet-like intercellular pattern, although in some patients we will observe a pattern of granular deposits on the cell surface of keratinocytes. There is also deposition of C3 in the biopsies of these patients, although, compared to IgG deposits, these deposits are always of lower intensity and found mostly in the lower layers of the epidermis. In general, most studies have shown that DIF is positive in more that 90 % of cases of PV, being more sensitive than indirect immunofluorescence (IIF) examination. Although all these findings are characteristic of PV, they cannot be considered specific as they may also be seen in any type of pemphigus (PF, PNP). Besides the importance in the diagnosis of PV, DIF has also been suggested as a useful marker to decide whether it is advisable to discontinue treatment in a patient in clinical remission. If, despite the absence of clinical lesions, DIF positivity persists when we perform a biopsy from normal skin, there is an increased risk of recurrence compared to patients with negative DIF in the same setting [41].
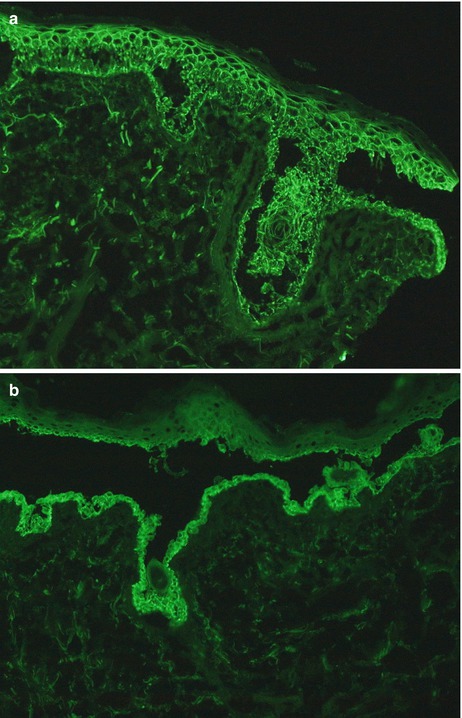
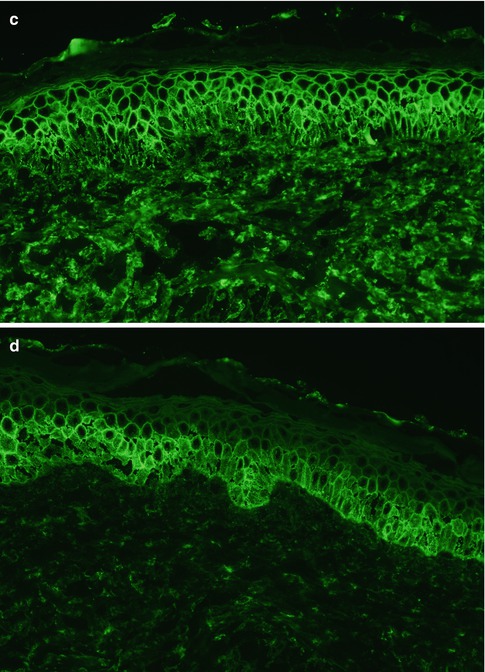
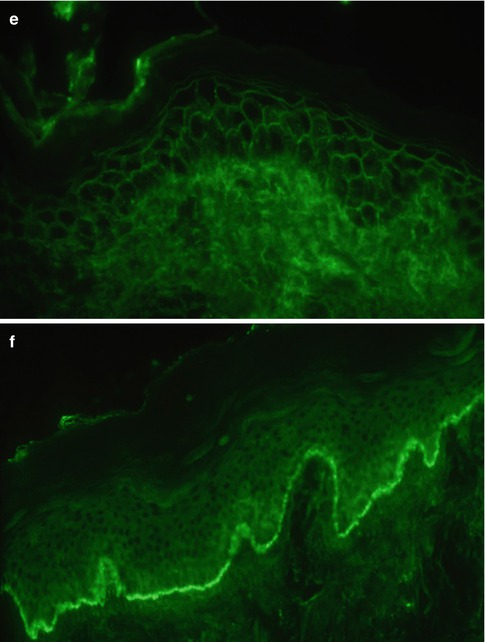
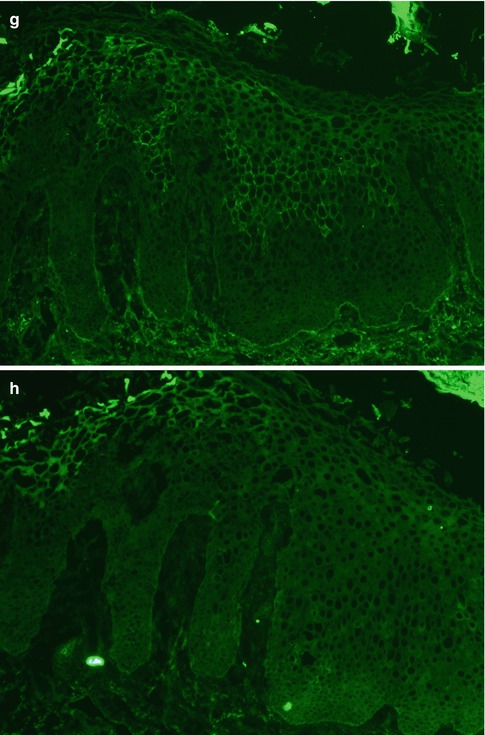
Fig. 16.4
(a) Pemphigus vulgaris, DIF for IgG. Direct immunofluorescence examination of the skin showing deposition of IgG on the cell surface of epidermal keratinocytes. A suprabasal intraepidermal blister can also be observed (original magnification ×200). (b) Pemphigus vulgaris, DIF for C3. Direct immunofluorescence examination of the skin from the same patient as in (a) showing deposition of C3 on the cell surface of epidermal keratinocytes of the lower epidermis. A suprabasal intraepidermal blister can also be observed (original magnification ×200). (c) Pemphigus foliaceus, DIF for IgG. Direct immunofluorescence examination of the skin showing deposition of IgG on the cell surface of epidermal keratinocytes of all the epidermis (original magnification ×200). (d) Pemphigus foliaceus, DIF for C3. Direct immunofluorescence examination of the skin from the same patient as in (d) showing deposition of C3 on the cell surface of epidermal keratinocytes of the lower epidermis. These deposits are less intense than the IgG deposits (original magnification ×200). (e) Paraneoplastic pemphigus, DIF for IgG. Direct immunofluorescence examination showing deposition of IgG on the cell surface of epidermal keratinocytes. This pattern is indistinguishable from other types of pemphigus (original magnification ×400). (f) Paraneoplastic pemphigus, DIF for C3. Direct immunofluorescence examination showing granular deposits of C3 along the basement membrane zone. This feature can be suggestive of paraneoplastic pemphigus, but can also be seen in other types of pemphigus (original magnification ×100). (g) IgA pemphigus, DIF for IgA. Direct immunofluorescence examination showing deposition of IgA on the cell surface of epidermal keratinocytes from the upper half of the epidermis (original magnification ×100). (h) IgA pemphigus, DIF for C3. Direct immunofluorescence examination from the same patient as in (g) showing negative staining for C3 (original magnification ×100)
Pemphigus Foliaceus and Erythematosus
In PF the characteristic DIF findings is the presence of IgG deposits on the keratinocyte cell surface in the outermost surface of the epidermis, sometimes extending to the upper two thirds of the stratum spinosum. In many patients there are also C3 deposits with the same distribution and pattern, although they are usually less intense. These findings may be similar to other types of pemphigus, like PV or PNP (Fig. 16.4c, d).
Pemphigus erythematosus (also known as Senear-Usher syndrome) was described originally as an overlap between PF and lupus erythematosus. These patients can present malar rash, positive antinuclear antibodies, and granular deposition of IgG and C3 along the BMZ (like a positive lupus band) besides the characteristic intercellular IgG deposits in the superficial layers of the epidermis. These findings are not specific of pemphigus erythematosus, as they may be not infrequently observed in PF, as well as in PNP, particularly the BMZ deposition of C3 [42]. What is less frequent is the finding of granular IgG deposition along the BMZ. It has been shown that this can occur after UV light exposure in patients with PF and that this might induce the cleavage of the desmoglein 1 ectodomain that co-localizes with IgG at the BMZ [43].
Paraneoplastic Pemphigus
DIF examination of perilesional skin in PNP can usually show the presence of IgG deposits on the cell surface of keratinocytes in the epidermis and adnexa with a similar pattern to other forms of pemphigus. There are also C3 deposits in the cell surface of keratinocytes, but they are usually less intense. Granular or linear deposits of immunoglobulins or C3 along the BMZ are also a frequent finding in PNP. They are usually of C3, but IgG may also be found, as well as IgA or IgM. This combined pattern (deposits on the surface of intercellular keratinocytes and in the BMZ) despite being suggestive of PPN is not very specific for the disease since it can be observed up to 10–20 % of other forms of pemphigus (primarily in pemphigus foliaceus, as described previously) [44] (Fig. 16.4e, f). In addition, between 20 and 60 % of PNP patients will have only an intercellular pattern that is indistinguishable from other forms of pemphigus, like PV [10]. In our personal experience, 57 % of biopsies from patients with PPN presented only intercellular deposits, while a combined pattern was observed only in 43 % of the biopsies. Another important fact in PPN is the high proportion of false-negative findings in DIF that have been reported in the literature (from 14 to 28 %) [45]. This false-negative rate in PPN is much higher than in other forms of pemphigus, and therefore, if there is a high clinical suspicion, a negative DIF does not exclude the diagnosis.
IgA Pemphigus
The diagnosis of IAP is mainly based on DIF findings. This shows the presence of intercellular IgA deposits in the epidermis. There are usually no other immunoreactants, and if they are found, the deposits are faint. The IgA deposits are usually located almost exclusively in the upper third of the epidermis in the subcorneal pustular dermatosis subtype, while in the intraepidermal neutrophilic dermatosis subtype, the intercellular deposits of IgA can be found throughout the epidermis, but sometimes they are more intense in the lower half (Fig. 16.4g, h).
16.2.1.2 Subepidermal Blistering Diseases
Bullous Pemphigoid
Biopsies from perilesional skin from patients with BP will show a typical DIF pattern with IgG and C3 deposition along the BMZ [46]. In most patients the deposits of C3 are more intense than those of IgG, and C3 deposits are found in 100 % of the patients, while IgG deposits in 70–80 % of the cases (Fig. 16.5a, b). In early stages, the deposition of immunoreactants can be exclusively of C3. In around 20 % of cases, there may be also deposits of IgM or IgA. Although this class of antibodies is not routinely studied by DIF, it has been shown that up to 40 % of patients with BP will present with linear deposits of IgE along the BMZ [47]. These IgE deposits have been related with the clinical presence of urticarial lesions in these patients and may be pathogenically related with the urticarial stage of BP.
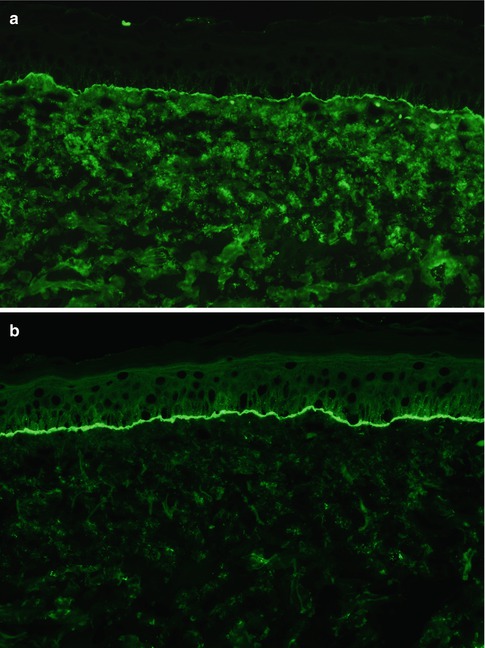
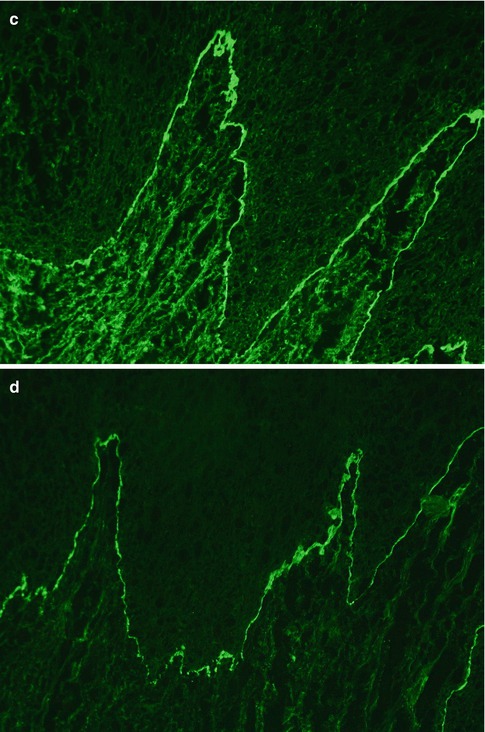
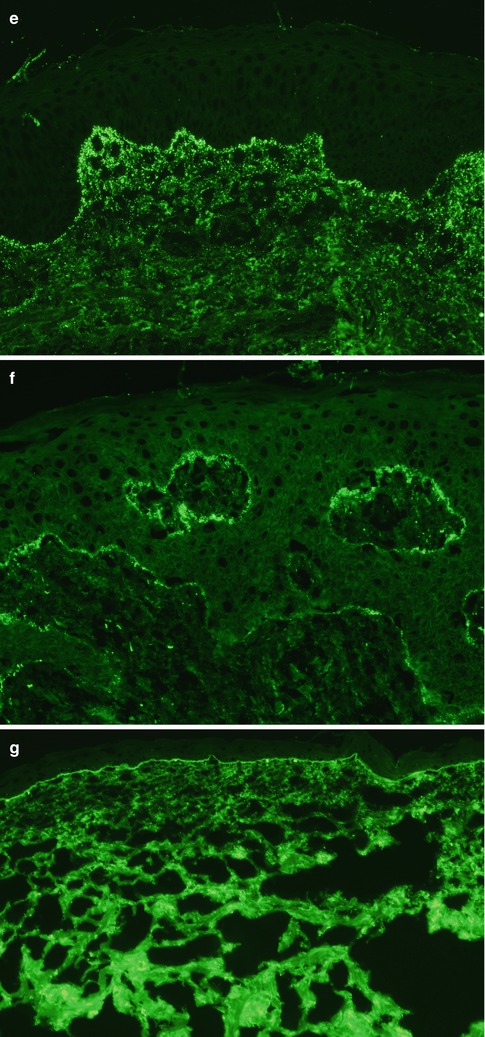
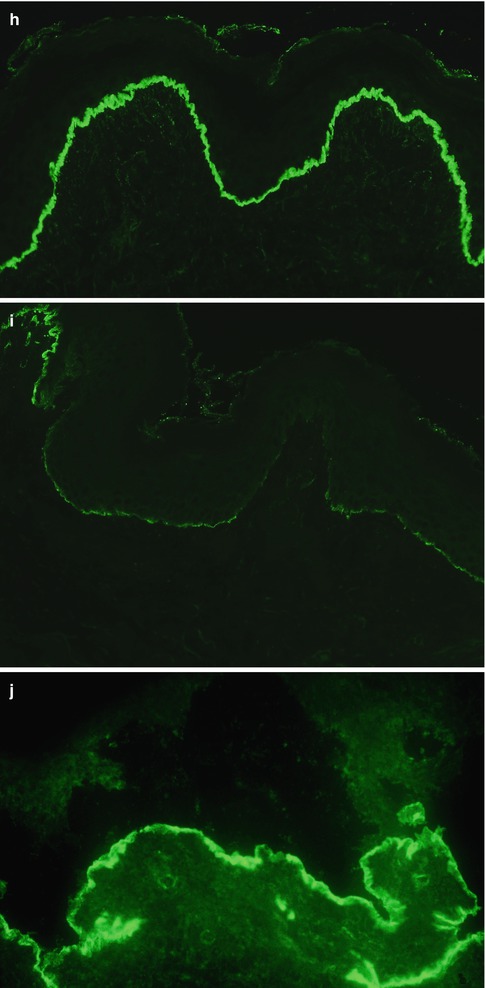
Fig. 16.5
 Kindlin-1 and Its Role in Kindler Syndrome
Kindlin-1 and Its Role in Kindler Syndrome
 Cyclophosphamide in Autoimmune Blistering Diseases: Safety, Efficacy and Evidence Base
Management of Bullous Systemic Lupus Erythematosus
Cyclophosphamide in Autoimmune Blistering Diseases: Safety, Efficacy and Evidence Base
Management of Bullous Systemic Lupus Erythematosus
 Using Intravenous Immunoglobulins in Autoimmune Bullous Diseases
Using Intravenous Immunoglobulins in Autoimmune Bullous Diseases
 Living with Epidermolysis Bullosa: Reviewing the Impact on Individuals’ Quality of Life
Living with Epidermolysis Bullosa: Reviewing the Impact on Individuals’ Quality of Life
 Dermatitis Herpetiformis
Dermatitis Herpetiformis




(a) Bullous pemphigoid, DIF for IgG. Direct immunofluorescence examination of the skin of a patient reveals linear lgG deposition along the basement membrane zone (original magnification ×200). (b) Bullous pemphigoid, DIF for C3. Direct immunofluorescence examination from the same patient as in (a) shows stronger linear C3 deposition along the basement membrane zone (original magnification ×200). (c) Mucous membrane pemphigoid, DIF for IgG. Direct immunofluorescence examination of the oral mucosa of a patient reveals linear lgG deposition along the basement membrane zone (original magnification ×200). (d) Mucous membrane pemphigoid, DIF for C3. Direct immunofluorescence examination of the oral mucosa from the same patient as in (c) shows also linear C3 deposition along the basement membrane zone (original magnification ×200). (e) Dermatitis herpetiformis, DIF for IgA. Direct immunofluorescence examination of the skin shows granular lgA deposition along the basement membrane zone, with a stronger positivity at the tips of the dermal papillae (original magnification ×100). (f) Dermatitis herpetiformis, DIF for C3. Direct immunofluorescence examination of the skin shows granular C3 deposits along the basement membrane zone (original magnification ×200). (g) Linear IgA bullous dermatosis, DIF for IgA. Direct immunofluorescence examination of the skin from a patient with vancomycin-induced linear IgA bullous dermatosis shows linear lgA deposition along the basement membrane zone (original magnification ×40). (h) Epidermolysis bullosa acquisita, DIF for IgG. Direct immunofluorescence examination of the skin of a patient demonstrates intense linear lgG deposition along the basement membrane zone (original magnification ×200). (i) Epidermolysis bullosa acquisita, DIF for C3. Direct immunofluorescence examination from the same patient as in (h) shows faint linear C3 deposition along the basement membrane zone (original magnification ×200). (j) Bullous systemic lupus erythematosus, DIF for IgG. Direct immunofluorescence examination of lesional skin demonstrates intense linear lgG deposition along the dermal side of the basement membrane zone (original magnification ×400)
Related posts:
Kindlin-1 and Its Role in Kindler Syndrome
Cyclophosphamide in Autoimmune Blistering Diseases: Safety, Efficacy and Evidence Base
Management of Bullous Systemic Lupus Erythematosus
Using Intravenous Immunoglobulins in Autoimmune Bullous Diseases
Living with Epidermolysis Bullosa: Reviewing the Impact on Individuals’ Quality of Life
Dermatitis Herpetiformis
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
